Assessment Measures
Assessment MeasuresA number of instruments have been developed to measure ACT and CBS processes. This section of the site will provide more information about these instruments, including downloads when available.
We encourage developers to contribute updates to this section of the site as often as possible. Interested parties are also encouraged to join the ACT for Professionals listserv and to read the Journal of Contextual Behavioral Science (JCBS) to learn of updated measures. Click on an instrument below to learn more about it.
ACBS Members: If you have an CBS specific measure you would like listed here, please email it and its reference citation to community@contextualscience.org
CBS Assessment Measures in 49 Languages Other than English
CBS Assessment Measures in 49 Languages Other than EnglishThis page includes a list of non-English measures relevant to ACT or psychological flexibility, or to other CBS-related areas (e.g., CFT, FAP, RFT, etc), both translated and original. As a courtesy, if you use these versions in research it is common to contact the translator (or originator if it began as a non-English measure) and let them know of the study -- ideally before publishing it. If you know of a non-English CBS-relevant measure validated in a journal or study, please email the instrument and the citation to community@contextualscience.org. The measures need not be limited to self-report measures validated by psychometric evaluations (indeed, psychometrics itself has been roundly criticized in the CBS literature). The measures can include experience sampling, behavioral, observational or other measures appropriate for idiographic functional analysis or idionomic process-based research, in line with the Task Force report on CBS research strategies (which you can find here: bit.ly/ACBSTaskForce). Thank you to all of our ACBS members who have contributed to this site, our science, and our community!
Measures in Albanian (Shqip)
Measures in Albanian (Shqip) CommunityMeasures in Arabic (اللغة العربية)
Measures in Arabic (اللغة العربية)Measures in Basque (Euskara)
Measures in Basque (Euskara) CommunityMeasures in Bosnian (Bosanski)
Measures in Bosnian (Bosanski) CommunityMeasures in Bulgarian (български)
Measures in Bulgarian (български) CommunityMeasures in Catalan (Català)
Measures in Catalan (Català) CommunityMeasures in Chinese (中文)
Measures in Chinese (中文)- AADQ - Chinese
- AAQ-II - Chinese
- AAQ-AHL - Chinese
- AFQ-Y8 - Chinese
- ASQ - Chinese
- ATQ - Chinese
- BEAQ - Chinese
- BI-AAQ - Chinese
- Brief COPE - Chinese
- CAMM - Chinese
- CAQ - Chinese
- CFQ - Chinese
- COPE - Chinese
- CPAQ - Chinese
- CompACT - Chinese
- DERS - Chinese
- ELS - Chinese
- FFMQ - Chinese
- FMI - Chinese
- KIMS - Chinese
- MAAS - Chinese
- MAAS-A - Chinese
- MEQ - Chinese
- MEQ-C - Chinese
- MPFI - Chinese
- PHLMS - Chinese
- PIPS - Chinese
- PPFI - Chinese
- PPFQ - Chinese
- Psy-Flex - Chinese
- SACS - Chinese
- SCS - Chinese
- SCS-SF - Chinese
- TAS-20 - Chinese
- VQ - Chinese
- WAAQ - Chinese
- WBSI - Chinese
- WSSQ - Chinese
Measures in Croatian (Hrvatski)
Measures in Croatian (Hrvatski) CommunityMeasures in Czech (Čeština)
Measures in Czech (Čeština)Measures in Danish (Dansk)
Measures in Danish (Dansk) CommunityMeasures in Dutch (Nederlandstalig)
Measures in Dutch (Nederlandstalig)- AAQ-II - Dutch
- AAQ-II-P - Dutch
- AAQ-ABI - Dutch
- AFQ-Y - Dutch
- ASQ - Dutch
- ATQ - Dutch
- Brief COPE - Dutch
- CAMM - Dutch
- CAQ - Dutch
- CEAS - Dutch
- CFQ - Dutch
- COPE - Dutch
- ELS - Dutch
- FFMQ - Dutch
- FIT-60 - Dutch
- FMI - Dutch
- KIMS - Dutch
- MAAS - Dutch
- MAAS-A - Dutch
- MEAQ - Dutch
- PIPS - Dutch
- Psy-Flex - Dutch
- SCS-SF - Dutch
- TAS-20 - Dutch
- WBSI - Dutch
Measures in Estonian (Eesti keel)
Measures in Estonian (Eesti keel) CommunityMeasures in Finnish (Suomi)
Measures in Finnish (Suomi)- AAQ-II - Finnish
- CPAQ - Finnish
- DERS - Finnish
- MAAS - Finnish
- Psy-Flex - Finnish
- TAS-20 - Finnish
- WBSI - Finnish
Click here for Arviointilomakkeet
- AAQ-II
- AFQ-Y
- ATQ
- CAMM
- CompACT
- DAAS
- FFMQ
- RISP
- VLQ
- WBSI
Measures in French (Français)
Measures in French (Français)- AAQ- II - French
- AAQ-SA - French
- ASQ - French
- ATQ - French
- Brief COPE - French
- CAMM - French
- CAQ-8 - French
- CFQ - French
- DERS - French
- EACQ - French
- FFMQ - French
- FMI - French
- KIMS - French
- MAAS - French
- MPFI - French
- PIPS - French
- Psy-Flex - French
- SCS - French
- TAS-20 - French
- VAAS - French
- WSSQ - French
Click here for more translations in French
- VLQ
- WBSI
Measures in Georgian (ქართული)
Measures in Georgian (ქართული) CommunityMeasures in German (Deutsch)
Measures in German (Deutsch)- AADQ - German
- AAQ-II - German
- AAQ-II-P - German
- ACT-SQ - German
- ASQ - German
- ASQ-Y - German
- BEAQ - German
- Brief COPE - German
- Bulls Eye - German
- CAQ - German
- CFQ - German
- CPAQ - German
- CTAQ - German
- CompACT - German
- DERS - German
- EQ - German
- FFMQ - German
- FMI - German
- KIMS - German
- MAAS - German
- PBAT - German
- PIPS - German
- Psy-Flex - German
- PVQ II - German
- SCS - German
- SCS-CA - German
- TAS-20 - German
- WBSI - German
- WSSQ - German
MPFI - German
MPFI - GermanMultidimensional Psychological Flexibility Inventory - German (MPFI-G, v1.0, 2/2022)
Quellenhinweis: Rolffs, J. L., Rogge, R. D., & Wilson, K. G. (2016). Disentangling Components of Flexibility via the Hexaflex Model Development and Validation of the Multidimensional Psychological Flexibility Inventory (MPFI). Assessment, 1073191116645905.
Deutsche Bearbeitung von K. Ackermann
Measures in Greek (Ελληνικά)
Measures in Greek (Ελληνικά)- AAQ-II - Greek
- AFQ-Y - Greek
- AIS - Greek
- BI-AAQ - Greek
- Brief COPE - Greek
- Bulls Eye - Greek
- CAMM - Greek
- CAQ-8 - Greek
- CFQ - Greek
- COPE - Greek
- CPAQ - Greek
- DERS - Greek
- KIMS - Greek
- MAAS - Greek
- MEQ - Greek
- PIPS - Greek
- Psy-Flex - Greek
- SCS - Greek
- SCS-Y - Greek
- TAS-20 - Greek
- VLQ - Greek
- VQ - Greek
Measures in Gujarati (ગુજરાતી)
Measures in Gujarati (ગુજરાતી) CommunityMeasures in Hebrew (עברית)
Measures in Hebrew (עברית) CommunityMeasures in Hindi (हिन्दी)
Measures in Hindi (हिन्दी) CommunityMeasures in Hungarian (Magyar)
Measures in Hungarian (Magyar)Measures in Icelandic (Íslenska)
Measures in Icelandic (Íslenska) CommunityMeasures in Indonesian (Bahasa Indonesia)
Measures in Indonesian (Bahasa Indonesia) CommunityMeasures in Italian (Italiano)
Measures in Italian (Italiano)- AAQ-II - Italian
- AAQ-Sports - Italian
- AFQ-Y - Italian
- ATQ - Italian
- Brief COPE - Italian
- CAMM - Italian
- CFQ - Italian
- CompACT - Italian
- COPE - Italian
- CPAQ - Italian
- CTAQ - Italian
- CVD-AAQ - Italian
- DERS - Italian
- FFMQ - Italian
- FMI - Italian
- ISS - Italian
- MAAS - Italian
- MAAS-A - Italian
- MEQ - Italian
- MFPI - Italian
- PBAT - Italian
- PHLMS - Italian
- PIPS - Italian
- Psy-Flex - Italian
- SCS - Italian
- SCS-SF - Italian
- TAS-20 - Italian
- VLQ - Italian
- WBSI - Italian
-
WSSQ - Italian
Miscellaneous Measures - Italian
Miscellaneous Measures - ItalianBVI Italian
BVI ItalianBaroni, D., McCracken, L. M., Matera, C., Nerini, A., & Stefanile, C. (2019). Misurare i valori: proprietà psicometriche della versione italiana del Brief Values Inventory. Psicoterapia Cognitiva e Comportamentale, 25(1), 13-33.
CTAQ - Italian Validation
CTAQ - Italian ValidationMoschen, R., Fioretti, A., Eibenstein, A., Natalini, E., Chiarella, G., Viola, P., Cuda, D., Cassandro, C., Scarpa, A., Rumpold, G., & Riedl, D. (2019). Validation of the Chronic Tinnitus Acceptance Questionnaire (CTAQ-I): the Italian version. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale, 39(2), 107–116. https://doi.org/10.14639/0392-100X-2144
DAS Italian
DAS ItalianDysfunctional Attitude Scale (DAS)
Weissman, A. & Beck, A. T. (1978). Development and validation of the dysfunctional attitudes scale. Paper presented at the meeting of the Association ot the Advancement of Behavior Therapy, Chicago, IL.
Referenza bibliografica: Melchiorri, E., Rossi, E., Panzera, A., Carloni, V., Romitelli, M., Picchio, G. (2015). Validation of the Dysfunctional Attitude Scale (DAS) in the Italian youth population. Poster presented at ACBS World Conference 13 Poster Session – Berlin, German- July 14-19, 2015.
Il presente studio è in corso di aggiornamento.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
PSS Italian
PSS ItalianPerceived Stress Scale (PSS-10)
Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health: Claremont Symposium on applied social psychology. Newbury Park, CA: Sage.
Referenza bibliografica: Melchiorri, E., Rossi, E., Panzera, A., Ristè, N., Carloni, V. (2015). Reliability and validity of an Italian version of the Perceived Stress Scale (PSS) for Youths. Poster presented at ACBS World Conference 13 Poster Session – Berlin, German- July 14-19, 2015.
Il presente studio è in corso di aggiornamento.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
SHS Italian
SHS ItalianSubjective Happiness Scale (SHS)
Lyubomirsky, S., & Lepper, H. S. (1999). A measure of subjective happiness: preliminary reliability and construct validation. Social Indicators Research, 46, 137-155.
Referenza bibliografica: Panzera., A., Carloni, V., Romitelli M., Rossi, E., Melchiorri, E. (2015). Subjective Happiness Scale (SHS): psychometric properties on an Italian sample of adolescents. Poster presented at ACBS World Conference 13 Poster Session – Berlin, German- July 14-19, 2015.
Il presente studio è in corso di aggiornamento.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
Measures in Japanese (日本語)
Measures in Japanese (日本語)- 6-PAQ - Japanese
- AAQ-II - Japanese
- AADQ - Japanese
- AFQ-Y - Japanese
- ASQ - Japanese
- ATQ - Japanese
- BEAQ - Japanese
- CAMM - Japanese
- Brief COPE - Japanese
- CEAS - Japanese
- CFQ - Japanese
- COPE - Japanese
- CPAQ - Japanese
- DERS - Japanese
- EACQ - Japanese
- EQ - Japanese
- FFMQ - Japanese
- MAAS - Japanese
- MPFI - Japanese
- PAAQ - Japanese
- PIPS - Japanese
- PVQ II - Japanese
- SCS - Japanese
- SCS-SF - Japanese
- SSCS - Japanese
- TAAQ - Japanese
- TAS-20 - Japanese
- TAQ - Japanese
- VLQ - Japanese
- VQ - Japanese
- WAAQ - Japanese
- WBSI - Japanese
The ACBS Japan Chapter website has more accessment tools.
- TSSQ
- VOYAGE
- VCQ
Measures in Korean (조선말, 한국어)
Measures in Korean (조선말, 한국어)- AAQ-II - Korean
- AAQ- S - Korean
- AFQ-Y - Korean
- ASQ - Korean
- BEAQ - Korean
- BIPIS - Korean
- Brief COPE - Korean
- CAQ - Korean
- CFQ - Korean
- CPAQ - Korean
- CPVI - Korean
- DERS - Korean
- ELS - Korean
- FFMQ - Korean
- ISS - Korean
- KIMS - Korean
- MAAS - Korean
- MEAQ - Korean
- MEQ - Korean
- PAQ - Korean
- Psy-Flex - Korean
- SA-AAQ - Korean
- SCS - Korean
- TAS-20 - Korean
- VLQ - Korean
- VQ - Korean
Measures in Latvian (Latviešu)
Measures in Latvian (Latviešu) CommunityMeasures in Lithuanian (Lietuvių kalba)
Measures in Lithuanian (Lietuvių kalba) CommunityMeasures in Macedonian (македонски)
Measures in Macedonian (македонски) CommunityMeasures in Malay (Bahasa Melayu)
Measures in Malay (Bahasa Melayu) CommunityMeasures in Montenegrin (Crnogorski)
Measures in Montenegrin (Crnogorski) CommunityMeasures in Norwegian (Norsk)
Measures in Norwegian (Norsk)Measures in Persian/Farsi (فارسی)
Measures in Persian/Farsi (فارسی)- AADQ - Persian
- AAQ-II - Persian
- AAQ-OC - Persian
- AAQ-W - Persian
- AFQ-Y - Persian
- ATQ - Persian
- BAFT - Farsi
- BI-AAQ - Persian
- BIPIS - Persian
- Brief COPE - Persian
- CAMM - Persian
- CAQ-8 - Persian
- CFQ - Persian
- CFQ-CI - Persian
- CompACT - Persian
- CPAQ - Persian
- DAAS - Persian
- DERS - Persian
- FFMQ - Persian
- FMI - Persian
- KIMS - Persian
- MAAS-A - Persian
- MEAQ - Persian
- MEQ - Persian
- MPFI - Persian
- PHLMS - Persian
- PIPS - Persian
- PFEQ - Persian
- PFSS - Persian
- PPFI - Persian
- SA-AAQ - Persian
- SCS - Persian/Farsi
- SCS-SF - Persian
- SCS-Y - Persian
- TAS-20 - Persian/Farsi
- VLQ - Persian
- VQ - Persian
- WSSQ - Persian
Measures in Polish (Polski)
Measures in Polish (Polski)Measures in Portuguese (Português)
Measures in Portuguese (Português)- 6-PAQ - Portuguese
- AAQ-II - Portuguese
- AAQ-EX - Brazilian Portuguese
- AAQ-SA - Portuguese
- AAQ-TS - Portuguese
- AAQ-US - Portuguese
- AAQ-W - Brazilian Portguese
- AFQ-Y - Portuguese
- ATQ - Portuguese
- BI-AAQ - Brazilian Portuguese
- Brief COPE - Portuguese
- CAMM - Portuguese
- CAQ-8 - Portuguese
- CFQ - Portuguese
- CFQ-BI - Brazilian Portuguese
- CFQ-CI - Portuguese
- CISS - Portuguese
- COPE - Portuguese
- CPAQ - Portuguese
- CompACT - Portuguese
- DERS - Portuguese
- ELS - Portuguese
- EQ - Brazilian Portuguese
- FAAQ - Brazilian Portuguese
- FFMQ - Portuguese
- FMI - Brazilian Portuguese
- ISS - Portuguese
- MAAS - Portuguese
- MEQ - Brazilian Portuguese
- MPFI - Portuguese
- PAAQ - Portuguese
- PHLMS - Brazilian
- PIPS - Portuguese
- PIS-I - Portuguese
- Psy-Flex - Portuguese
- PsyFlex-A - Portuguese Version
- SA-AAQ - Portuguese
- SCS - Portuguese
- SCS-A - Portuguese
- SCS-SF - Portuguese
- SEQ - Portuguese
- TA-AAQ-A - Portuguese
- TAAQ - Portuguese
- TAS-20 - Portuguese
- VAAS - Portuguese
- VLQ - Portuguese
- VQ - Portuguese
- WAAQ - Portuguese
- WBSI - Portuguese
Measures in Romanian (Română)
Measures in Romanian (Română)Measures in Russian (Русский)
Measures in Russian (Русский) CommunityMeasures in Serbian (Српски)
Measures in Serbian (Српски) CommunityMeasures in Sinhala (සිංහල)
Measures in Sinhala (සිංහල) CommunityMeasures in Slovak (Slovenskej)
Measures in Slovak (Slovenskej) CommunityMeasures in Slovenian (Slovenščina)
Measures in Slovenian (Slovenščina)Measures in Somali (Af Soomaali)
Measures in Somali (Af Soomaali) CommunityMeasures in Spanish (Español)
Measures in Spanish (Español)- 6-PAQ - Spanish
- AAQ-II - Spanish
- AAQ-S - Spanish
- AAQ-SA - Spanish
- AAQ-US - Spanish
- AAQ-W - Spanish
- ACRS - Spanish
- ACT-FM - Spanish
- AFQ-Y - Spanish
- ATQ - Spanish
- BAFT - Spanish
- BEAQ - Spanish
- BI-AAQ - Spanish
- Brief COPE - Spanish
- Bull's Eye - Spanish
- CAMM - Spanish
- CAQ-8 - Spanish
- CFQ - Spanish
- CompACT - Spanish
- COPE - Spanish
- CPAQ - Spanish
- DERS - Spanish
- EACQ - Spanish
- EAS - Spanish
- ELS - Spanish
- EOSS - Spanish
- EQ - Spanish
- FAAQ - Spanish
- FFMQ - Spanish
- FMI - Spanish
- GPQ - Spanish
- KIMS - Spanish
- LSI - Spanish
- MAAS - Spanish
- MAAS-A - Spanish
- MPFI - Spanish
- PAAQ - Spanish
- PHLMS - Spanish
- PIPS - Spanish
- Psy-Flex - Spanish
- PVQ-II - Spanish
- SCS - Spanish
- SCS-SF - Spanish
- SSCS - Spanish
- TAS-20 - Spanish
- VLQ - Spanish
- VQ - Spanish
- WAAQ - Spanish
- WAM-C/A - Spanish
- WBSI - Spanish
Miscellaneous Measures - Spanish
Miscellaneous Measures - Spanish CommunityBADS Spanish
BADS SpanishBarraca, J., Pérez-Álvarez, M., & Lozano, J.H. (2011). Avoidance and Activation as Keys to Depression: Adaptation of the Behavioral Activation for Depression Scale in a Spanish Sample. The Spanish Journal of Psychology, 14 (2). (http://dx.doi.org/10.5209/rev_SJOP.2011.v14.n2.45).
Reasons for Living Inventory (Inventario de Razones para Vivir)
Reasons for Living Inventory (Inventario de Razones para Vivir)Traducido de Chiles, J. A., Strosahl, K. D., & Roberts, L. W. (2019). Clinical Manual for Assessment and Treatment of Suicidal Patients. 2nd Edition. American Psychiatric Association Publishing.
Suicide Risk Scale (Escala de Riesgo Suicida)
Suicide Risk Scale (Escala de Riesgo Suicida)Traducido de Chiles, J. A., Strosahl, K. D., & Roberts, L. W. (2019). Clinical Manual for Assessment and Treatment of Suicidal Patients. 2nd Edition. American Psychiatric Association Publishing.
Measures in Swedish (Svenska)
Measures in Swedish (Svenska)- 6-PAQ - Swedish
- AAQ-II - Swedish
- AAQ-W - Swedish
- ACT Advisor - Swedish
- AFQ-Y - Swedish
- ASQ - Swedish
- Bulls Eye - Swedish
- CAQ - Swedish
- CEAS - Swedish
- CFQ - Swedish
- CPAQ - Swedish
- CPVI - Swedish
- CompACT - Swedish
- DERS - Swedish
- FFMQ - Swedish
- HAQ - Swedish
- KIMS - Swedish
- MAAS - Swedish
- MPFI - Swedish
- PFSS - Swedish
- PIPS - Swedish
- PPFQ - Swedish
- Psy-Flex - Swedish
- SCS - SF - Swedish
- TAS-20 - Swedish
- VAAS - Swedish
- VQ - Swedish
- WAAQ - Swedish
- WBSI - Swedish
Measures in Tamil (தமிழ்)
Measures in Tamil (தமிழ்) CommunityMeasures in Thai (ภาษาไทย)
Measures in Thai (ภาษาไทย) CommunityMeasures in Turkish (Türkiye)
Measures in Turkish (Türkiye)- AADQ - Turkish
- AAQ-II - Turkish
- AAQ-SA - Turkish
- AAQ-US - Turkish
- ASQ - Turkish
- ATQ - Turkish
- CAMM - Turkish
- CFQ - Turkish
- COPE - Turkish
- CPAQ - Turkish
- DDS - Turkish
- DERS - Turkish
- ELS - Turkish
- EQ - Turkish
- FFMQ - Turkish
- FMI - Turkish
- FoReST - Turkish
- MAAS - Turkish
- MAAS-A - Turkish
- MEAQ - Turkish
- MEQ - Turkish
- MEQ-C - Turkish
- MPFI - Turkish
- PHLMS - Turkish
- Psy-Flex - Turkish
- SA-AAQ - Turkish
- SCS - Turkish
- SCS-Y - Turkish
- TAS-20 - Turkish
- TPFS - Turkish
- VAAS - Turkish
- VLQ - Turkish
- VQ - Turkish
- WBSI - Turkish
- WAAQ - Turkish
- WSSQ - Turkish
- Translations in Turkish: CPAQ-R, CPVI, PIPS, BI-AAQ, AAQ-TS
- More Transalations in Turkish: DAAS, AFQ-Y
Go to the ACBS Türkiye Chapter website for more measures
AAQW-R
AAQW-RBeing overweight, a severe public health problem, is associated with experiential avoidance. This study aims to examine the reliability and validity of the Turkish version of the Acceptance and Action Questionnaire for weight-revised (AAQW-R) in people with a BMI above 25. The sample consisted of 169 participants with a Body Mass Index (BMI) above 25. The participants who gave informed consent were asked to fill out a demographic form, AAQW-R (Acceptance and Action Questionnaire-2), AAQ-2, Weight Self- Stigma Questionnaire (WSSQ), and General Health Questionnaire (GHQ). Internal consistency and item-total correlation were evaluated using Cronbach’s alpha coefficient. Cronbach’s alpha coefficient was used to test the factor structure. The temporal stability was assessed with the test-retest method. AAQW-R has significant correlations with BMI, AAQ-2, WSSQ, and GHQ. CFA demonstrates a three- factor structure (χ2=57.0, df=31; RMSEA=0.0714; RMSEA 90% CI lower bond=0.0411, RMSEA 90% CI upper bond=0.100, CFI=0.968; TLI=0.954). AAQW-R and subscales of AAQW-R have significant correlations with AAQ-2, AAQW-R, BMI, WSSQ, and GHQ (p<0.05). Correlation analysis stated temporal stability for all items in Spearman correlation analyses (p<0.05). According to the results of this study, AAQW-R is a reliable and valid scale that can measure experiential avoidance in the context of psychological flexibility among overweight and obese people.
Measures in Ukrainian (українська)
Measures in Ukrainian (українська) CommunityMeasures in Urdu (اردو)
Measures in Urdu (اردو)Measures in Vietnamese (Tiếng Việt)
Measures in Vietnamese (Tiếng Việt) CommunityReviews of Measures
Reviews of Measures CommunityMeasuring ACT in context: Challenges and future directions (2023)
Measuring ACT in context: Challenges and future directions (2023)Ong, C,.W., Sheehan, K.G., Haaga, D.A.F. (2023) Measuring ACT in context: Challenges and future directions. Journal of Contextual Behavioral Science, 28, 235-247. https://doi.org/10.1016/j.jcbs.2023.04.005
Measures Reviewed: CompACT, CFQ, PPFI, Psy-Flex, IRAP, ELS, Values Wheel, VLQ, MPFI, EPIC, OESQ, TOF, GPQ, PBAT, ACT-FM, AAQ-II and AAQ variants
Abstract: Measurement in acceptance and commitment therapy (ACT) should prioritize theoretically relevant outcomes (well-being, values-consistent action) and hypothesized processes of change (psychological flexibility and its components). Development and refinement of ACT measures have proceeded rapidly and with some success. This review describes empirical research on such issues as measurement invariance in diverse samples and identifies challenges associated with measurement of key ACT constructs such as psychological (in)flexibility and values. Important priorities for future research include continued evaluation of discriminant validity of psychological inflexibility measures from general distress as well as more frequent incorporation of multiple assessment modalities including non-self-report methods. Recommendations for ACT measurement in clinical practice include anchoring assessment in values and personalizing assessment to the client.
The Relationship Between Psychological Inflexibility and Well-Being in Adults: A Meta-Analysis of the Acceptance and Action Questionnaire (2023)
The Relationship Between Psychological Inflexibility and Well-Being in Adults: A Meta-Analysis of the Acceptance and Action Questionnaire (2023)Ong, C.W., Barthel, A.L., & Hofmann, S.G. (2023). The Relationship Between Psychological Inflexibility and Well-Being in Adults: A Meta-Analysis of the Acceptance and Action Questionnaire. Behavior Therapy. https://doi.org/10.1016/j.beth.2023.05.007
Measures Reviewed: AAQ and its variants
Abstract
Psychological inflexibility is defined as the rigid responding to stimuli (e.g., unpleasant thoughts and feelings) that interferes with well-being and valued actions. It is the treatment target in acceptance and commitment therapy (ACT). Despite the centrality of the link between inflexibility and well-being to ACT theory, an empirical review clarifying the nature of this relationship has not been conducted. As such, the current meta-analysis examined the meta-correlation between psychological inflexibility, measured by the Acceptance and Action Questionnaire (AAQ) and its variants, and well-being. A systematic review yielded 151 studies, including 25 versions of the AAQ and 43 well-being measures. Consistent with ACT theory, higher psychological inflexibility was associated with worse well-being (r = −.47, 95% CI[−.49, −.45]). In addition, sample diagnosis, type of AAQ, and type of well-being measure significantly moderated this relationship. Overall, our findings support the hypothesized link between psychological inflexibility and worse well-being. Limitations include reliance on cross-sectional data, precluding causal interpretation.
Discussion
The present meta-analysis examined the relationship between psychological inflexibility, measured by the AAQ and its variants, and well-being, variously defined as quality of life, life satisfaction/flourishing, and valued action. Based on 262 correlation coefficients reported from 151 studies across over 35 countries and 22 languages, the overall correlation between psychological inflexibility and well-being was −.47, 95% CI[−.49, −.45]...
A psychometric validation of contextual cognitive behavioral therapy-informed measures with racially and ethnically diverse adults (2022)
A psychometric validation of contextual cognitive behavioral therapy-informed measures with racially and ethnically diverse adults (2022)Spencer, S.D., Jo, D., Hamagami, F., Antonio, M.C.K., Qinaʻau, J., Masuda, A., & Hishinuma, E.S. (2022). A psychometric validation of contextual cognitive behavioral therapy-informed measures with racially and ethnically diverse adults. Journal of Contextual Behavioral Science, 25, 61-72. https://doi.org/10.1016/j.jcbs.2022.06.004
Measures Reviewed: FFMQ, ELS, and AAQ-II
Abstract
The Five Facet Mindfulness Questionnaire (FFMQ), Engaged Living Scale (ELS), and Acceptance and Action Questionnaire-II (AAQ-II) are three commonly used contextual cognitive behavioral therapy (CBT)-informed self-report questionnaires. The present study aimed to psychometrically validate these three scales with racially and ethnically diverse adults in Hawaiʻi (N = 1102). Using a cross-validation strategy with an iterative process of exploratory and confirmatory factor analyses, findings revealed that factor structures of the FFMQ, ELS, and AAQ-II were theoretically consistent with extant literature. However, we also found slight factorial structure differences in the present sample, which may have practical implications when assessing these constructs within racially and ethnically diverse adults. Evidence of reliability, convergent validity, and measurement invariance of these scales are also provided. Implications and limitations of these findings are discussed.
Measuring psychological flexibility in autistic adults: Examining the validity and reliability of the AAQ-II, BEAQ, and VQ (2022)
Measuring psychological flexibility in autistic adults: Examining the validity and reliability of the AAQ-II, BEAQ, and VQ (2022)Aller T.B., Barrett, T., Levin, M.E., Brunson McClain, M. (2022). Measuring psychological flexibility in autistic adults: Examining the validity and reliability of the AAQ-II, BEAQ, and VQ. Journal of Contextual Behavioral Science, 26, 125-133. https://doi.org/10.1016/j.jcbs.2022.09.001
Measures Reviewed: AAQ-II, BEAQ, and VQ
Abstract:
Autistic adults, adults who have an autism spectrum disorder diagnosis, are more likely than their non-autistic peers to experience mental health concerns. A growing body of literature supports interventions that target psychological flexibility as a useful approach for reducing mental health concerns in autistic adults. Despite this, psychometric evidence on measuring psychological flexibility within this population is scant. Accordingly, we determined the validity and reliability of the Acceptance and Action Questionnaire-II (AAQ-II), Brief Experiential Avoidance Questionnaire (BEAQ), and Valuing Questionnaire (VQ) in measuring psychological flexibility in a sample of 461 autistic adults. Each of the measures demonstrated consistent factor structures and internal consistency as was proposed in the original measurement development articles. Convergent, discriminant, and explanatory validity of the AAQ-II, BEAQ, and VQ aligned with a priori hypotheses. The AAQ-II, BEAQ and VQ obstruction subscale demonstrated redundancy in one another suggesting the benefits of selecting a single measure of psychological flexibilty for research. The VQ Progress subscale demonstrated more explanatory validity for key mental health outcomes compared to the other measures. Overall, the VQ scale might be the most useful of the three measures in measuring psychological flexibility in autistic adults in clinical settings, but each included scale appeared reliable and valid for this population.
Defining and measuring “psychological flexibility”: A narrative scoping review of diverse flexibility and rigidity constructs and perspectives (2021)
Defining and measuring “psychological flexibility”: A narrative scoping review of diverse flexibility and rigidity constructs and perspectives (2021)Cherry, K.M., Vander Hoeven, E., Patterson, T.S., & Lumley, M.N. (2021). Defining and measuring “psychological flexibility”: A narrative scoping review of diverse flexibility and rigidity constructs and perspectives. Clinical Psychology Review, 84, 101973. https://www.sciencedirect.com/science/article/abs/pii/S0272735821000167
12 measures were reviewed including the AAQ-II and PPFI.
Abstract:
Psychological flexibility (PF) is a popular construct in clinical psychology. However, similar constructs have existed since the mid-20th century, resulting in different terms, definitions and measures of flexibility, hindering the advancement of the field. The main measure of PF – the Acceptance and Action Questionnaire (AAQ-II; Bond et al., 2011) – has also been heavily criticized. To move towards definitional consensus and improved measurement, we surveyed the literature to map PF and related-terms, examine definitional overlaps, and assessthe psychometric quality of prominent flexibility measures. A scoping review was conducted in two databases (PsycNET and SCOPUS). Twenty-three flexibility constructs appeared across 220 articles, and twelve measures were included and rated for quality. PF, psychological inflexibility (PI), and cognitive flexibility (CF) were most prominent. Definitional similarities among prominent flexibility constructs emerged, namely handling distress or interference, taking action, and meeting goals or values. The Personalized Psychological Flexibility Index (PPFI; Kashdan, Disabato, Goodman, Doorley, & McKnight, 2020) appears to be the best measure available to assess PF. Problems with the current use of the AAQ-II were apparent, hindering current knowledge of PF. Definitional consensus and measurement development are vital to advance the field. To this end, recommendations and next steps for researchers and practitioners are outlined.
A multicultural examination of experiential avoidance: AAQ – II measurement comparisons across Asian American, Black, Latinx, Middle Eastern, and White college students (2020)
A multicultural examination of experiential avoidance: AAQ – II measurement comparisons across Asian American, Black, Latinx, Middle Eastern, and White college students (2020)Borgogna, N.C., McDermott, R.C., Berry, A., Lathan, E.C., & Gonzales, J. (2020). A multicultural examination of experiential avoidance: AAQ – II measurement comparisons across Asian American, Black, Latinx, Middle Eastern, and White college students. Journal of Contextual Behavioral Science, 16, 1-8. https://doi.org/10.1016/j.jcbs.2020.01.011
Measures reviewed: AAQ – II
Abstract
Experiential avoidance is a common psychological process, a core component of third-wave behavioral therapies, and a robust predictor of general psychopathology. The Acceptance and Action Questionnaire (AAQ version II [AAQ – II]; Bond et al. 2011) is a popular and widely used measure of experiential avoidance. However, studies examining the measurement and function of the AAQ-II across cultures are largely relegated to translational investigations across different languages, thus providing little information about measurement equivalence among English speaking populations from different racial/ethnic backgrounds. The present study examined data from the 2016–2017 National Healthy Minds Study (HMS; N = 24,439) and tested the measurement invariance of the AAQ – II across White, Black, Latinx, Asian American, and Middle Eastern college students. We then examined how racial/ethnic group moderated experiential avoidance as a concurrent predictor of anxiety and depression. Multigroup structural equation modeling indicated support for configural but not metric measurement invariance across all groups. The effect size of the non-invariance was small in magnitude. The AAQ – II functioned as a strong positive correlate of anxiety and depression measures across racial/ethnic groups. Moderation analyses further indicated that the AAQ-II was a significantly stronger predictor of anxiety and depression for White participants (β′s = .717, .738 respectively) compared to Asian American participants (β′s = 0.671, 0.665 respectively) and was a significantly stronger predictor of anxiety for White participants compared to Latinx respondents (β = 0.662). Implications for research, theory, and clinical practice are discussed, with specific recommendations for culturally informed adaptations to the AAQ – II.
A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance (2020)
A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance (2020)A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance
Ong, C.W., Pierce, B.G., Petersen, J.M., Barney, J.L., Fruge, J.E., Levin, M.E., & Twohig, M.P. (2020). A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance. Journal of Contextual Behavioral Science, 18, 34-47. https://doi.org/10.1016/j.jcbs.2020.08.007
Measures Reviewed: AAQ-II, AAQ-3 (revised AAQ-II), BEAQ, and CompACT
Abstract:
Psychological inflexibility is a rigid behavioral pattern that interferes with engagement in personally meaningful activities; it is the hypothesized root of suffering in acceptance and commitment therapy (ACT). Thus, the quality of its measurement affects the research, theory, and practice of ACT. The current study aimed to evaluate the discriminant validity and item performance of four measures of psychological inflexibility: the Acceptance and Action Questionnaire—II (AAQ-II), a revised version of the AAQ-II (AAQ-3), the Brief Experiential Avoidance Questionnaire (BEAQ), and the Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT). We analyzed data from community (n = 253), student (n = 261), and treatment-seeking samples (n = 140) using exploratory factor analysis and multigroup graded-response models. The CompACT had the strongest discriminant validity followed by the AAQ-3, whereas items in the CompACT Behavioral Awareness and Valued Action subscales performed most consistently across groups. No single measure emerged as clearly superior to others; rather, appropriate selection of measures depends on the goals and context of assessment. Scientific and clinical implications are discussed.
JCBS Special Issue on ACT Process Measurement (2019)
JCBS Special Issue on ACT Process Measurement (2019)In the Journal of Contextual Behavioral Science Volume 12, Maria Karekla and Nuno Ferreira guest edited the Special Issue on ACT Process Measurement. ACBS members can read the Special Issue on ACT Process Measurement in the JCBS portal.
The JCBS Special Issue on ACT Process Measurement contains 16 articles:
- A review of AAQ variants and other context-specific measures of psychological flexibility
- A systematic review of values measures in acceptance and commitment therapy research
- Assessing psychological flexibility: Validation of the Open and Engaged State Questionnaire
- Assessing psychological inflexibility in hoarding: The Acceptance and Action Questionnaire for Hoarding (AAQH)
- Assessing psychological inflexibility in university students: Development and validation of the acceptance and action questionnaire for university students (AAQ-US)
- Assessing the valuing process in Acceptance and Commitment Therapy: Experts' review of the current status and recommendations for future measure development
- Development and initial validation of the Generalized Pliance Questionnaire
- Further validation of the Chronic Pain Acceptance Questionnaire for Adolescents in a broader paediatric context
- Network analysis: A new psychometric approach to examine the underlying ACT model components
- Preliminary psychometric properties of the Everyday Psychological Inflexibility Checklist
- Preliminary validation and reliability assessment of a 10-item Tacting of Function Scale
- Psychometric properties of acceptance measures: A systematic review
- Psychometric properties of the Avoidance and Fusion Questionnaire – Youth in Colombia
- Scaling-up assessment from a contextual behavioral science perspective: Potential uses of technology for analysis of unstructured text data
- The Acceptance and Action Questionnaire-II (AAQ-II) as a measure of experiential avoidance: Concerns over discriminant validity
-
The initial validation of a state version of the Cognitive Fusion Questionnaire
A review of AAQ variants and other context-specific measures of psychological flexibility (2019)
A review of AAQ variants and other context-specific measures of psychological flexibility (2019)Ong, C. W., Lee, E.B., Levin, M.E., & Twohig, M.T. (2019). A review of AAQ variants and other context-specific measures of psychological flexibility. Journal of Contextual Behavioral Science, 12, 329-346. https://doi.org/10.1016/j.jcbs.2019.02.007
Measures Reviewed: AAQ-II and AAQ-II variants, 6-PAQ, BIPIS, CPAQ, PPF
Abstract:
Psychological flexibility refers to a way of interacting with internal experiences and the external environment that advances one toward chosen values whereas psychological inflexibility reflects rigid adherence to ineffective responses such that valued living is compromised. Psychological flexibility is a critical variable of interest in acceptance and commitment therapy, thus, accurate assessment of this construct is pertinent to professionals in the field. Numerous measures of psychological flexibility for specific conditions exist and the psychometric validation of each of these measures varies in breadth and depth. To orient professionals to the scope of available measures as well as their psychometric properties, the current review summarizes the existing literature on context-specific measures of psychological flexibility. Most measures demonstrated satisfactory basic psychometric properties, though their clinical utility (e.g., treatment sensitivity) has largely been underexplored. Generally, context-specific measures performed better than a generic measure of psychological flexibility with respect to incremental validity and treatment sensitivity. Still, further research is needed to validate these measures (e.g., discriminant validity) in order to justify their use across settings and study designs.
A systematic review of values measures in acceptance and commitment therapy research (2019)
A systematic review of values measures in acceptance and commitment therapy research (2019)Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
Measures Reviewed: BEVS, CPVI, ELS, VLS, VLQ, VQ
Absract:
Values are a guiding principle in Acceptance and Commitment Therapy (ACT), and a vital element of both ACT research and clinical assessment. This systematic review aimed to evaluate the current evidence for the utility and efficacy of quantitative survey measures that assess values within an ACT study framework. Online databases were searched using key words to identify research articles administering values-based assessments. A thorough database search yielded 65 separate articles that met inclusion criteria, and eight validated scales measuring values. Value-scale psychometric studies that met inclusion criteria were assessed for content validity, internal consistency, and construct validity. Results provide information to guide future researchers regarding the most psychometrically sound and appropriate measures that assess values across multiple criteria. While the measures vary significantly in psychometric properties, the Valuing Questionnaire, the Engaged Living Scale (either short or long form), and the Valued Living Scale appear to have the strongest methodological support. Important future directions include further psychometric studies across all measures to assess their utility in more diverse contexts (e.g., randomized controlled trials, time-lagged, and other controlled studies of ACT treatment) and populations (e.g., age, health, race, ethnicity, nationality, etc.) with consideration of a measure's definition of values within an ACT context.
Psychometric properties of acceptance measures: A systematic review (2019)
Psychometric properties of acceptance measures: A systematic review (2019)McAndrews, Z., Richardson, J., & Stopa, L. (2019) Psychometric properties of acceptance measures: A systematic review. Journal of Contextual Behavioral Science, 12, 261-277. DOI: 10.1016/j.jcbs.2018.08.006
Measures Reviewed: AAQ, AAQ-II, FFMQ, FFMQ-15, PHLMS, KIMS, DERS, S-DERS, ASQ
Abstract:
Acceptance is an important construct across models for understanding psychological distress. Several measures have been designed to capture this, however, there is a lack of evidence regarding the most suitable tool. The objective of this review was to systematically evaluate measurement properties of tools designed to measure self-reported acceptance. A systematic review of the literature on psychometric properties of acceptance measures was performed. Articles were selected if the primary aim was to develop or evaluate measurement properties (validity, reliability, responsiveness) of a self-report acceptance scale (or subscale). The methodological quality of included studies was evaluated using the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) checklist. The quality of measurement properties were evaluated using criteria suggested by Terwee et al. (2007). All studies were independently reviewed by two raters, and inter-rater reliability was assessed. The search strategy identified 3097 unique articles. Twenty articles, reporting 32 studies, met inclusion criteria. Nine instruments were identified; two unidimensional scales of acceptance, four mindfulness tools with an acceptance subscale, and three emotion regulation scales with an acceptance-based subscale. None of the instruments were assessed across all domains of psychometric properties. No studies investigated measurement error or cross-cultural validity. Internal consistency was the most widely assessed property, and was generally acceptable across all scales. Lack of target population involvement resulted in poor content validity for most scales. Inter-rater reliability of study selection and evaluation was excellent. There are important conceptual differences across current acceptance measures, which might result from differences in theoretical models on which these are based. None of the measures evaluated can be recommended as having superior psychometric properties. Important limitations in content validity need to be addressed, with greater involvement of target populations. Further research is required to demonstrate the psychometric properties of existing measures, given their significant role in evaluating acceptance-based interventions across clinical and research settings.
It's all about the process: Examining the convergent validity, conceptual coverage, unique predictive validity, and clinical utility of ACT process measures (2019)
It's all about the process: Examining the convergent validity, conceptual coverage, unique predictive validity, and clinical utility of ACT process measures (2019)Rogge, R.D., Daks, J.S., Dubler, B.A., & Saint, K.J. (2019) It's all about the process: Examining the convergent validity, conceptual coverage, unique predictive validity, and clinical utility of ACT process measures. Journal of Contextual Behavioral Science, 14, 90-102. https://doi.org/10.1016/j.jcbs.2019.10.001
Measures Reviewed: AAQ-II, CompACT, MPFI, OESQ.
Abstract
The Acceptance and Commitment Therapy (ACT) literature now offers a range of process measures, including: the Acceptance and Action Questionnaire-II (AAQ-II), the Open and Engaged State Questionnaire (OESQ), the Comprehensive Assessment of ACT Processes (CompACT), and the Multidimensional Psychological Flexibility Inventory (MPFI). The current study sought to directly compare and contrast the information provided by those scales: (1) in a sample of 2,385 online respondents (67% female, 85% Caucasian, M = 33yo) and (2) in a case study of a client receiving ACT for a depressive disorder. Quantitative results revealed that all of the flexibility scales were strongly linked to wellbeing whereas the inflexibility scales were strongly linked to psychological distress. The results further highlighted that newer multidimensional scales (the 3-dimension CompACT, the 12-dimension MPFI) offered greater insights into current functioning, often doubling the amount of variance explained by the AAQ-II alone. Both the quantitative analyses and the clinical case study demonstrate the more nuanced and clinically meaningful patterns that emerge when multiple dimensions of flexibility and inflexibility are tracked. In particular, the results suggested the MPFI (and the online MindFlex Assessment System that makes the MPFI easy to administer and interpret) offers researchers and clinicians the most conceptually comprehensive scale to assess the dimensions of the Hexaflex model. Implications for clinical research and practice are discussed.
A Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (2019)
A Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (2019)Barrett, K., O’Connor, M. & McHugh, L. A (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
Measures Reviewed: VQ, ELS, VLQ, MPFI, AAQ-OC, BEVS
Abstract:
The ACT model consists of acceptance, cognitive defusion, contact with the present moment, self-as-context, values, and committed action, which together create psychological flexibility. Limited research has examined the unique contribution of values-focused work in acceptance-based therapies. To investigate this in a reliable and valid way, it is critical to ensure that the instruments used to measure values are empirically sound. This review aims to identify value-based psychometric tools currently in use, and examine their ability to reliably and validly measure the ACT-defined concept of values. The current study searched PsycINFO, Medline, and PubMed databases for psychometric validation papers of values-measurement instruments. Seventeen values-measures were evaluated by extracting data relating to their content, structural, construct, convergent, and discriminant validity, as well as internal consistency and test–retest reliability. The COSMIN manual for systematic reviews of Patient-Reported Outcome Measures (PROMs) was utilized as a guideline for assessing bias and examining the quality of psychometric tools identified. Outcomes suggest that the Valuing Questionnaire (Smout, Davies, Burns, & Christie, 2014), Engaged Living Scale (Trompetter et al., 2013), Valued Living Questionnaire (Wilson, Sandoz, Kitchens, & Roberts, 2010), Multidimensional Psychological Flexibility Inventory (Rolffs, Rogge, & Wilson, 2018), Acceptance and Action Questionnaire for Obsessions and Compulsions (Jacoby, Abramowitz, Buchholz, Reuman, & Blakey, 2018), and Bulls-Eye Values Survey (Lundgren, Luoma, Dahl, Strosahl, & Melin, 2012) have the best psychometric properties. A number of alternative values-based instruments demonstrate preliminary evidence for their utility, though further examination of these is necessary. This review also highlights a number of issues pertaining to the cohesiveness and psychometric comprehensiveness of current values-measurement research, with recommendations for improvement.
Probing the relative psychometric validity of three measures of psychological inflexibility (2018)
Probing the relative psychometric validity of three measures of psychological inflexibility (2018)Renshaw, T.L. (2018). Probing the relative psychometric validity of three measures of psychological inflexibility. Journal of Contextual Behavioral Science, 7, 47-54. https://doi.org/10.1016/j.jcbs.2017.12.001
Measures Reviewed: AAQ-II, AFQ-Y8, and AFQ-Y17
Abstract:
The present study probed the relative structural and concurrent validity of responses to three self-report measures of psychological inflexibility with a large sample of college students (N = 797): the revised version of the Acceptance and Action Questionnaire (AAQ-II), the shorter version of the Avoidance and Fusion Questionnaire for Youth (AFQ-Y8), and the longer version of the Avoidance and Fusion Questionnaire for Youth (AFQ-Y17). Structural validity findings showed that responses to the AAQ-II and AFQ-Y8 indicated good data–model fit and latent construct reliability, whereas the data–model fit for responses to the AFQ-Y17 was poor, despite strong latent construct reliability. Concurrent validity findings demonstrated that scores derived from all three measures of psychological inflexibility had comparable correlations with several concurrent indicators of negative mental health (i.e., depression, anxiety, global negative affect), positive mental health (i.e., happiness, hope, global positive affect), and theoretically-similar therapeutic processes (i.e., mindfulness skills). Yet findings from hierarchical regressions evidenced some incremental validity when scores from the AAQ-II, AFQ-Y8, and AFQ-Y17 were taken together to predict concurrent mental health outcomes—suggesting potential differential construct representation among these three measures. Limitations of the present study and future directions for research and practice are discussed.
Measuring Mindfulness in Youth: Review of Current Assessments, Challenges, and Future Directions (2017)
Measuring Mindfulness in Youth: Review of Current Assessments, Challenges, and Future Directions (2017)Goodman, M.S., Madni, L.A. & Semple, R.J. Measuring Mindfulness in Youth: Review of Current Assessments, Challenges, and Future Directions. Mindfulness, 8, 1409–1420 (2017). https://doi.org/10.1007/s12671-017-0719-9
7 measures were reviewed including CAMM and MAAS-A
Abstract
Interest in mindfulness-based interventions (MBIs) for youth continues to grow across academic, clinical, educational, and community settings. Conclusions regarding the effects of mindfulness training with youth are tempered by methodological issues. One common limitation is the availability of reliable and valid ways to measure mindfulness. This review identifies existing youth mindfulness measures, discusses key challenges to measurement, and offers suggestions for improving assessment research. A search of electronic databases, consultation with colleagues, and data from professional meetings yielded seven self-report measures: (a) Child and Adolescent Mindfulness Measure (CAMM); (b) Mindful Attention Awareness Scale for Adolescents (MAAS-A); (c) Mindful Attention Awareness Scale for Children (MAAS-C); (d) Comprehensive Inventory of Mindfulness Experiences-Adolescents (CHIME-A); (e) Mindful Thinking and Action Scale for Adolescents (MTASA); (f) Mindfulness Scale for Pre-Teens, Teens, and Adults (MSPTA); and (g) Mindfulness Inventory for Children and Adolescents (MICA). All seven assess trait mindfulness through self-report. We discuss methodological concerns regarding the near-exclusive use of self-report measures to assess youth mindfulness and offer suggestions for validating new measures and improving research studies that incorporate the assessment of mindfulness in youth.
A Review of ACT-measures (2015)
A Review of ACT-measures (2015)In October 2015 our systematic review on available ACT-measures (+ 50!) was published in the Dutch Journal of Psychiatry (“New generation behaviour therapy; new generation assessment measures; a review of currently available assessment measures”). Of course, we would like to share our findings with the international CBS-community as well; so we decided to post a brief excerpt of the relevant finding here on the ACBS-website, hoping this could be of use to this community (see attachment below for the full-overview).
Warm regards,
Tim Batink
T. BATINK, G. JANSEN, F.P.M.L. PEETERS
BACKGROUND
Acceptance and Commitment Therapy (ACT) is a relatively new form of behaviour therapy, which has Relational Frame Theory (RFT) as its theoretical foundation. Since ACT is not aimed primarily at reducing psychopathological symptoms, changes are likely to be needed in the nature and purpose of the assessment measures used.
AIM
To provide an up-to-date overview of ACT-measures that are suitable for use with adults and that will assist clinicians and researchers.
METHOD
We performed a systematic review of the literature.
RESULTS
More than 50 ACT-related questionnaires were identified; which will be listed per ACT-component (supplemented with reference).
CONCLUSION
Clinicians and researchers with an interest in ACT have many measures at their disposal. Most of these are available free of charge.
SHORT EXCERPT
In October 2015, a systematic review on available ACT-measures was published in the Dutch Journal of Psychiatry. The current document serves as a brief excerpt of the relevant findings for the international community. We began this review with searches in ACT oriented sources: the website of the Association for Contextual Behavioral Science (ACBS; http://contextualscience.org), the mailing list of the ACBS and Journal of Contextual Behavioral Science (JCBS). As search terms 'questionnaire', 'scale' and 'test' were used. Subsequently, we applied this same approach in the PubMed with 'acceptance' and 'commitment' as additional search terms. This resulted in 58 questionnaires (February 2015). Below, we will give an overview of these questionnaires, classified per ACT-component and specific problem areas / disorders. Additionally, a list with the full-names of the questionnaires with a core-reference will be provided, completed with a full reference list. Please use to reference below, when citing this overview.
Original source: Batink, T., Jansen, G., & Peeters, F. (2015). Nieuwe generatie gedragstherapie, nieuwe generatie meetinstrumenten; een overzicht van beschikbare ACT-meetinstrumenten [New generation behaviour therapy; new generation assessment measures; a review of currently available assessment measures]. Tijdschrift voor Psychiatrie, 57, 739-748.
Author correspondence: Tim Batink (tim.batink@maastrichtuniversity.nl)
ACT Measures Packet (2006)
ACT Measures Packet (2006)Compiled by Joseph Ciarrochi & Linda Bilich.
Ciarrochi, J., & Bilich, L. (2006). Acceptance and Commitment Therapy. Measures Package: Process measures of potential relevance to ACT. Unpublished manuscript, University of Wollongong, Australia.
(attached below)
Table of Contents:
Forward .................................................................................................... ......................... 3
Avoidance / Acceptance .................................................................................................... 4
The Acceptance and Action Questionnaire (AAQ-2) ......................................................... 5
White Bear Suppression Inventory (WBSI) ....................................................................... 8
Emotion Control Questionnaire (ECQ2) .......................................................................... 15
State Social Anxiety and State Emotion-Regulation Questionnaires ............................... 19
Repressive Defensive Coping ........................................................................................... 22
Miller Behavioral Style Scale (MBSS)............................................................................. 28
Experiential Avoidance Scale ........................................................................................... 31
Balanced Inventory of Desirable Responding (BIDR) ..................................................... 35
Fusion / Dysfunctional thinking..................................................................................... 38
Automatic Thoughts Questionnaire (ATQ) ...................................................................... 39
Personal Need for Structure (PNS) ................................................................................... 42
Belief in Personal Control Scale (BPCS) ......................................................................... 44
Dysfunctional Attitude Scale (DAS) ................................................................................ 48
Narcissistic Personality Inventory (NPI) .......................................................................... 51
Rosenberg Self-Esteem Scale (RSE) ................................................................................ 53
Adult Dispositional Hope Scale........................................................................................ 55
Adult State Hope Scale .................................................................................................... . 57
Domain Specific Hope Scale (DSHS) .............................................................................. 59
Sociotropy – Autonomy Scale (SAS) ............................................................................... 64
Mindfulness / Awareness of feelings ................................................................................ 70
Kentucky Inventory of Mindfulness Skills (KIMS) ......................................................... 71
The Mindfulness Attention Awareness Scale (MAAS).................................................... 74
Value clarification / Goal striving / Action orientation ............................................... 77
Personal Strivings Assessment ......................................................................................... 78
Valued Living Questionnaire (VLQ) ................................................................................ 95
The BULLs-eye Instrument about valued life Primary Care Version (BULLI-PC) ........ 98
The Bulls-eye Instrument about valued life.................................................................... 103
Action Control Scale (ACS-90) ...................................................................................... 109
Pleasant Events Schedule............................................................................................ .... 114
ACT measures for specific populations ...................................................................... 126
Diabetes Acceptance and Action Scale for Children and Adolescents (DAAS) ............ 127
Avoidance and Fusion Questionnaire for Youth (AFQ-Y) ............................................ 131
Child Acceptance and Mindfulness Measure (CAMM) ................................................. 133
Chronic Pain Acceptance Questionnaire – Revised (CPAQ-R) ..................................... 136
Chronic Pain Values Inventory (CPVI) .......................................................................... 138
Psychological Inflexibility in Pain Scale (PIPS) ............................................................ 141
Trauma Specific AAQ (AAQ-TS) .................................................................................. 143
ACT weekly Diary .................................................................................................... ...... 147
Child and Adolescent Measures
Child and Adolescent MeasuresThis page contains a working list of child and adolescent specific measures related to ACT processes.
Avoidance and Fusion Questionnaire for Youth (AFQ-Y)
Avoidance and Fusion Questionnaire for Youth (AFQ-Y)The AFQ was derived from an initial pool of 50 items developed to measure psychological acceptance, conceptualized as an active and multidimensional process involving high or low levels of: willingness to experience private events, values-oriented action, experiential avoidance, and cognitive and emotional fusion. Results of exploratory factor analysis on these initial 50 items supported a three-factor solution. Factor one consisted of 25 items, all negatively worded. Conceptually, this factor seems to tap into experiential avoidance and fusion and is now the Avoidance and Fusion Questionnaire for Youth (AFQ-Y).
We have used the AFQ with children and adolescents 9-17 years old. Based on results from school studies in middle Tennessee, children report good comprehension of items. The AFQ seems to be a stronger predictor of negative outcomes such as physical and emotional symptoms.
The AFQ-Y is on ruthbaer.com.
Citations:
Greco, L. A., Lambert, W., & Baer, R. A. (2008). Psychological inflexibility in childhood and adolescence: Development and evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychological Assessment, 20(2), 93–102. https://doi.org/10.1037/1040-3590.20.2.93
Livheim, F., Tengström, A., Bond, F.W., Andersson, G., Dahl, J. & Rosendahl, I. (2016). Psychometric properties of the Avoidance and Fusion Questionnaire for Youth: A psychological measure of psychological inflexibility in youth. Journal of Contextual Behavioral Science, 5(2), 103-110. https://doi.org/10.1016/j.jcbs.2016.04.001
Renshaw, T.L. (2018). Probing the relative psychometric validity of three measures of psychological inflexibility. Journal of Contextual Behavioral Science, 7, 47-54. https://doi.org/10.1016/j.jcbs.2017.12.001
AFQ-Y - Czech
AFQ-Y - CzechSuchardová, S. (2023). Krátká intervence ACT jako preventivní program ke zvýšení kognitivní flexibility u žáků středních škol. Thesis: Univerzita Palackého v Olomouci. Retrieved from https://theses.cz/id/yz2xvg/Suchardova__DP.pdf The AFQ-Y Czech version is in the appendix.
AFQ-Y - Dutch Version
AFQ-Y - Dutch VersionKrimmel, K.L. (2015) Het meten van psychologische flexibiliteit: een pilot onderzoek naar de psychometrische eigenschappen van de avoidance and fusion questionnaire bij volwassen patiënten die een bariatrische ingreep ondergaan. Thesis, Universiteit of Twente. The Dutch AFQ-Y is at the end of the article.
Blokzijl, R. (2005). Measuring Acceptance-Related Constructs Among Youngsters: Evaluation of the Dutch Willingness and Action Measure for Children and Adolescents (WAM-C/A) and the Avoidance and Fusion Questionnaire for Youth (AFQ-Y). Thesis, University of Leiden.
Click here for het Nederlandse taalgebied vertaling gemaakt van de AFQ-Y.
AFQ-Y - Greek Validation
AFQ-Y - Greek ValidationChristodoulou, A., Michaelides, M. P., & Karekla, M. (2018). Greek Version of the Avoidance and Fusion Questionnaire for Youth: Psychometric Evaluation and Gender Multigroup Invariance in Adolescents. Journal of Psychoeducational Assessment, 36(8), 844–849. https://doi.org/10.1177/0734282917713500
Abstract
The Avoidance and Fusion Questionnaire for Youth–Eight-Item Short Version (AFQ-Y8) assesses psychological inflexibility in youth. The present study is the first to examine alternative measurement models for the Greek adaptation of the AFQ-Y8, latent associations with the Acceptance and Action Questionnaire–II (AAQ-II), gender-group invariance, and latent mean comparisons between males and females. In total, 432 students from seven high schools in Cyprus participated in the study. Both a unidimensional and a two-dimensional model had excellent fit, although the one-factor solution was substantively superior. The correlation of the latent AFQ-Y8 factor with AAQ-II was strong and positive, indicating good convergent validity. Finally, the unidimensional AFQ-Y8 model was found to be invariant for gender and no latent means difference was detected between males and females.
AFQ-Y - Italian
AFQ-Y - ItalianAvoidance and Fusion Questionnaire for Youth
Greco, L.A., Murrell, A.R., & Coyne, L.W. (2005). The Avoidance and Fusion Questionnaire for Youth. Available from the first author and online at www.contextualscience.org.
Greco, L.A., Lambert, W., & Baer, R.A. (2008). Psychological inflexibility in childhood and adolescence: Development and evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychological Assessment, 20(2), 93-102.
Traduzione Italiana (1.0) a cura di Rossi, E., Melchiorri, E., Francesconi, C., Violini, P., Cioci, M., Ristè, N. (2013) AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (2.0) a cura di Melchiorri, E., Rossi, E., Ristè, N., Violini, P., Lijoi, E., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Rossi, E., Melchiorri, E., Violini, P., Lijoi, E., Ristè, N., Panzera, A. (2014). Validation study of the Italian Version of the Avoidance and Fusion Questionnaire for Youth (AFQ-Y). Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014.
Schweiger, M., Ristallo, A., Oppo, A., Pergolizzi, F., Presti, G., & Moderato, P. (2017). Ragazzi in lotta con emozioni e pensieri: la validazione della versione italiana dell’ Avoidance and Fusion Questionnaire for Youth (I-AFQ-Y) [Youths struggling with emotions and thoughts: validation of the Italian version of the Avoidance and Fusion Questionnaire for Youth (I-AFQ-Y)]. Psicoterapia Cognitiva e Comportamentale, 23(2), 141–162.
Compare, L., Martucci, C., Bernini, O., Cincidda, C. & Berrocal, C. (2021) Proprietà psicometriche dell'Avoidance and Fusion Questionnaire for Youth (AFQ-Y) in soggetti di 6-11 anni [Psychometric properties of Avoidance and Fusion Questionnaire for Youth (AFQ-Y) in children aged between 6-11]. Psicoterapia Cognitiva e Comportamentale, 27(1), 45-63. https://doi.org/doi:10.14605/PCC2712103
Il presente studio è in corso di aggiornamento.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
AFQ-Y - Japanese
AFQ-Y - JapaneseAvoidance and Fusion Questionnaire for Youth (AFQ-Y) is a measure of the psychological inflexibility of adolescents from childhood to adolescence.
There are 17 items AFQ-Y and 8 items shortened version AFQ-Y8. AFQ-Y has a one-factor structure.
Ishizu, K., Shimoda, Y., & Ohtsuki, T. (2014) Developing the scale regarding psychological inflexibility in Japanese early adolescence.
Poster presented at 30th Annual Pacific Rim International Conference on Disability and Diversity, Honolulu
The AFQ-Y Japanese Version is on the ACBS Japan Chapter website.
AFQ-Y - Persian Adaptation
AFQ-Y - Persian AdaptationShabani, M., Mohsenabadi, H., Zanjani, Z., Assarian, F. (2019). Evaluation of psychometric properties of Persian version of Avoidance and Fusion Questionnaire for Youth (AFQ – Y). Journal of Fundamentals of Mental Health, 21(5), 325-333. http://doi.org/10.22038/jfmh.2019.14804
Hekmati, I. et al (2020) Persian adaptation of avoidance and fusion questionnaire for youth (AFQ-Y): A preliminary examination of its psychometric properties. Journal of Contextual Behavioral Science, 17, 46-54. https://doi.org/10.1016/j.jcbs.2020.05.004
AFQ-Y - Portuguese
AFQ-Y - PortugueseCunha, M. & Santos, A.M. (2011) Avaliação da Inflexibilidade Psicológica em Adolescentes: Estudo das qualidades psicométricas da versão portuguesa do Avoidance and Fusion Questionnaire for Youth (AFQ-Y). Laboratório de Psicologia, 9(2), 133-146. Retrieved from https://core.ac.uk/download/pdf/235397938.pdf
Cunha, M., Oliveira, S., Coimbra, M. et al. (2023). Assessing Psychological Inflexibility in Adolescents: A Validation Study of the Portuguese Short Version of the Avoidance and Fusion Questionnaire for Youth. Child Youth Care Forum, 52, 123–138. https://doi.org/10.1007/s10566-022-09679-9
AFQ-Y - Spanish Validation
AFQ-Y - Spanish ValidationSe presenta la versión española validada del Avoidance and Fusion Questionnaire for Youth (AFQ-Y).
El texto completo de la validación se puede encontrar en:
Valdivia-Salas, S., Martín-Albo, Zaldívar, P.J.L., Lombas, S., & Jiménez, T.I. (2017). Spanish validation of the Avoidance and Fusion Questionnaire for Youth. Assessment, 24(7), 919-931. https://doi.org/10.1177/1073191116632338
Salaza, D.M. et al (2019) Psychometric properties of the Avoidance and Fusion Questionnaire – Youth in Colombia. Journal of Contextual Behavioral Science, 12, 305-313. https://doi.org/10.1016/j.jcbs.2018.11.008
García-Rubio, C., Lecuona, O., Blanco Donoso, L. M., Cantero-García, M., Paniagua, D., & Rodríguez-Carvajal, R. (2020). Spanish validation of the short-form of the Avoidance and Fusion Questionnaire (AFQ-Y8) with children and adolescents. Psychological Assessment, 32(4), e15–e27. https://doi.org/10.1037/pas0000801
AFQ-Y - Swedish
AFQ-Y - SwedishDetta test mäter det psykologiska konstruktet ”psykologisk inflexibilitet”, eller dess motsats ”psykologisk flexibilitet” om man vänder på numreringen. Testet är framtaget för ungdomar 12-18 år. Men har även visat sig fungera bra för vuxna. Både AFQ-Y8 samt den längre versionen, AFQ-Y17 finns validerade för svenska förhållanden. I denna artikel finns testets psykometriska egenskaper beskrivna. En konklusion i denna artikel är att AFQ-Y8 är att föredra. I denna artikel summeras även all forskning internationell forskning som är gjord och vetenskapligt publicerad på AFQ-Y till och med januari 2016. Både forskning på unga och vuxna. Du hittar AFQ-Y8 här och AFQ-Y17 här.
Referenser:
[1] Livheim, F., Tengström, A., Bond, F. W., Gerhard Andersson, G., Dahl, J. & Rosendahl, I. (2016). Psychometric Properties of the Avoidance and Fusion Questionnaire for Youth: A Psychological Measure of Psychological Inflexibility in youth. Journal of Contextual Behavioral Science, 5(2), 103-110. https://doi.org/10.1016/j.jcbs.2016.04.001
Se länk till artikeln här.
[2] Thorsell Cederberg, J., Weineland, S., Dahl, J., Ljungman,G. (2018) A preliminary validation of the Swedish short version of the Avoidance and Fusion Questionnaire for Youth (AFQ-Y8) for children and adolescents with cancer. Journal of Contextual Behavioral Science, 10, 103-107. https://doi.org/10.1016/j.jcbs.2018.09.004
AFQ-Y8 - Chinese
AFQ-Y8 - ChineseChen Yanhong, Zhao Ying, Duan Yanmei, Bai Xiaoyu, Wang Shujuan, & Zhu Zhuohong. (2019). 青少年回避与融合问卷简版的信效度分析 [Reliability and validity analysis of the short version of the adolescent avoidance and fusion questionnaire]. Chinese Journal of Clinical Psychology, 27(6), 1192-1195, 1114.
AFQ-Y8 - Korean Validation
AFQ-Y8 - Korean ValidationSeong-Hye Choi (아주대학교), Eun-Jung Kim(아주대학교) (2016) Psychological Inflexibility in Korean Children and Adolescents : Validation of the Korean Version of the Avoidance and Fusion Questionnaire for Youth-Eight Item Type (K-AFQ-Y8). Korean Journal of Clinical Psychology, 35(3), 600 - 614.
Choi Seong-Hye, Kim Eun-Jeong (2015) Assessing Psychological Inflexibility in Childhood and Adolescence : Validation of the Korean Version of the Avoidance and Fusion Questionnaire for Youth(K-AFQ-Y). Congnitive Behavior Therapy in Korea, 15(3), 595 - 617.
AFQ-Y8- Turkish Version
AFQ-Y8- Turkish VersionBüyüköksüz, E., & Erözkan, A. (2019). Avoidance and Fusion Questionnaire –Youth 8 (AFQ-Y8): Factor Structure and Reliability Studies in Turkish Culture. Journal of Cognitive Behavioral Psychotherapy and Research. 8(Supplement 1): 3-7.
Büyüköksüz, E., & Erözkan, A. (2019). Kaçınma ve Birleşme Ölçeği-Gençler 8 (KBÖ-G8): Türk Kültüründe Faktör Yapısı ve Güvenirlik Çalışmaları. Journal of Cognitive Behavioral Psychotherapy and Research. 8(Supplement 1): 3-7.
Revised Avoidance & Fusion Questionnaire for Youth (AFQ-Y; Greco, Murrell, & Coyne, 2005)
Revised Avoidance & Fusion Questionnaire for Youth (AFQ-Y; Greco, Murrell, & Coyne, 2005)The Avoidance and Fusion Questionnaire for Youth (AFQ-Y; Greco, Murrell, & Coyne, 2005) is a 17-item measure that asks respondents to rate how true each item is for them (0 = Not at All True; 4 = Very True). Items are tied to ACT’s model of human suffering and were generated to represent a theoretically cohesive conceptualization of psychological inflexibility fostered by: (1) Cognitive fusion (e.g., “My thoughts and feelings mess up my life,” “The bad things I think about myself must be true”); (2) Experiential avoidance (e.g., “I push away thoughts and feelings that I don’t like”); and (3) Inaction or behavioral ineffectiveness in the presence of unwanted internal experiences (e.g., “I can’t be a good friend when I feel upset”).
Consistent with the theory underlying acceptance and commitment therapy (ACT), items converged into a 17-item scale (AFQ-Y) and an 8-item short form (AFQ-Y8). Results of classical test theory, factor analysis, and item response theory support the psychometric properties of the 17-item version of the AFQ-Y and AFQ-Y8. Overall, research suggests that the AFQ-Y may be a useful and child-friendly measure of core ACT processes.
Reference
Greco, L. A., Lambert, W., & Baer, R. A. (2008). Psychological inflexibility in childhood and adolescence: Development and evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychological Assessment, 20(2), 93-102.
Acceptance and Action Diabetes Questionnaire - Youth (AADQ-YR)
Acceptance and Action Diabetes Questionnaire - Youth (AADQ-YR)Berlin, KS, Keenan, ME, Cook, JL, et al. Measuring psychological flexibility in youth with type 1 diabetes. Pediatr Diabetes. 2020; 21: 1566– 1574. https://doi.org/10.1111/pedi.13110
AADQ-YR - Persian
AADQ-YR - PersianRajaeiramsheh, F., Rezaie, Z., Davoudi, M. et al. (2021) Psychometric properties of the Persian versions of acceptance and action diabetes questionnaire (AADQ) and the diabetes acceptance and action scale (DAAS), in Iranian youth with type 1 diabetes. J Diabetes Metab Disord, 20, 655–663. https://doi.org/10.1007/s40200-021-00796-1 The Persian version of the AADQ-YR is in the Supplementary Information.
Child and Adolescent Mindfulness Measure (CAMM)
Child and Adolescent Mindfulness Measure (CAMM)The Children's Acceptance and Mindfulness Measure is a 10-item measure of acceptance and mindfulness for youth. https://ruthbaer.com/academics/CAMM.pdf
Greco, L., Baer, R. A., & Smith, G. T. (2011). Assessing mindfulness in children and adolescents: Development and validation of the child and adolescent mindfulness measure (CAMM). Psychological Assessment, 23, 606-614.
Goodman, M.S., Madni, L.A. & Semple, R.J. (2017). Measuring Mindfulness in Youth: Review of Current Assessments, Challenges, and Future Directions. Mindfulness, 8, 1409–1420. https://doi.org/10.1007/s12671-017-0719-9
Prenoveau, J.M,, Papadakis, A.A., Schmitz, J.C.S., et al. (2018). Psychometric properties of the Child and Adolescent Mindfulness Measure (CAMM) in racial minority adolescents from low-income environments. Psychological Assessment, 30(10), 1395-1400. DOI: 10.1037/pas0000630
CAMM - Catalan Validation
CAMM - Catalan ValidationViñas, F., Malo, S., González, M., Navarro, D., & Casas, F. (2015). Assessing Mindfulness on a Sample of Catalan-Speaking Spanish Adolescents: Validation of the Catalan Version of the Child and Adolescent Mindfulness Measure. The Spanish journal of psychology, 18, E46. https://doi.org/10.1017/sjp.2015.48
CAMM - Chinese
CAMM - ChineseChen, X., Liang, K., Huang, L., Mu, W., Dong, W., Chen, S., Chen, S., & Chi, X. (2022).The Psychometric Properties and Cutoff Score of the Child and Adolescent Mindfulness Measure (CAMM) in Chinese Primary School Students. Children, 9(4), 499. https://doi.org/10.3390/children9040499
CAMM - Czech
CAMM - CzechSuchardová, S. (2023). Krátká intervence ACT jako preventivní program ke zvýšení kognitivní flexibility u žáků středních škol. Thesis: Univerzita Palackého v Olomouci. Retrieved from https://theses.cz/id/yz2xvg/Suchardova__DP.pdf The CAMM Czech version is in the appendix.
CAMM - Dutch Validity
CAMM - Dutch Validityde Bruin, E.I., Zijlstra, B.J.H. & Bögels, S.M. (2014). The Meaning of Mindfulness in Children and Adolescents: Further Validation of the Child and Adolescent Mindfulness Measure (CAMM) in Two Independent Samples from The Netherlands. Mindfulness 5, 422–430. https://doi.org/10.1007/s12671-013-0196-8
CAMM - French Validation
CAMM - French ValidationRoux, B., Franckx, A.-C. Lahaye, M., Deplus, S. & Philippot, P. (2019). A French validation of the Child and Adolescent Mindfulness Measure (CAMM). Revue Européenne de Psychologie Appliquée. 69(3), 83-89. http://doi.org/10.1016/j.erap.2019.06.001
Dion, J., Paquette, L., Daigneault, I., Godbout, N., & Hébert, M. (2018). Validation of the French Version of the Child and Adolescent Mindfulness Measure (CAMM) Among Samples of French and Indigenous Youth. Mindfulness, 9(2), 645–653. https://doi.org/10.1007/s12671-017-0807-x
Letellier, S. (2018) Validation du «Child and Adolescent Mindfulness Measure» (CAMM) et du «Acceptance and Fusion Questionnaire for Youth» (AFQ-Y) auprès d’enfants québécois de 8 à 12 ans. Université de Sherbrooke, Dissertation. Retrieved from https://savoirs.usherbrooke.ca/handle/11143/13577
The French CAMM is in Appendix D.
CAMM - Greek
CAMM - GreekTheofanous, A., Ioannou, M., Zacharia, M., Georgiou, S. N., & Karekla, M. (2020). Gender, Age, and Time Invariance of the Child and Adolescent Mindfulness Measure (CAMM) and Psychometric Properties in Three Greek-Speaking Youth Samples. Mindfulness, 110. https://doi.org/10.1007/s12671-020-01350-5
CAMM - Italian
CAMM - ItalianChildren's Acceptance and Mindfulness Measure
Greco, L. A., Smith, G., & Baer, R. A. (2009). Assessing mindfulness in children and adolescents: Development and validation of the Chidlren’s Acceptance and Mindfulness Measure (CAMM). Unpublished manuscript. St. Louis: University of Missouri.
Traduzione Italiana (2.0) a cura di Rossi, E., Melchiorri, E., Violini, P., Lijoi, E., Ristè, N.,(2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Melchiorri, E., Rossi, E., Ristè, N., Violini, P., Lijoi, E., Panzera, A. (2014). Development and validation study of the Italian Version of the Child and Adolescent Mindfulness Measure (CAMM . Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014.
Ristallo, A., Schweiger, M., Oppo, A. Pergolizzi, F. Presti, G. & Moderato, P. (2016). Misurare la mindfulness in età evolutiva: proprietà psicometriche e struttura fattoriale della versione italiana della Child and Adolescent Mindfulness Measure (I-CAMM). Psicoterapia Cognitiva e Comportamentale, 22. DOI: 10.1037/t61201-000.
Il presente studio è in corso di aggiornamento.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
CHILD AND ADOLESCENT MINDFULNESS MEASURE: ITALIAN VALIDATION (I-CAMM)
CHILD AND ADOLESCENT MINDFULNESS MEASURE: ITALIAN VALIDATION (I-CAMM)Attached you can find the Italian version of the Child and Adolescent Mindfulness Measure (I- CAMM). The instrument was validated on a sample of 1336 students (age range 11-18), from different part of Italy.
The psychometric properties, factor structure, normative data and scoring are discussed in our paper “Misurare la mindfulness in età evolutiva: proprietà psicometriche e struttura fattoriale della versione italiana della Child and Adolescent Mindfulness Measure (I-CAMM)” by Arianna Ristallo, Marta Schweiger, Annalisa Oppo, Francesca Pergolizzi, Giovambattista Presti e Paolo Moderato (Psicoterapia Cognitivo Comportamentale, in press). Below you can find the abstract:
The aim of this study is to analyze psychometric properties and factorial structure of the Italian version of the CAMM. Twelve schools were involved in the study and 1336 participants, aged between 11 and 18, were enrolled in two studies. The I-CAMM shows a two factors solution with a higher-order factor named “Mindfulness Skills”. The two factors detected are named “Awareness” and “Willingness”, respectively. The two factors solution is identified both with Exploratory Factor Analysis- performed on 657 participants recruited during the study 1 - and through the Confirmatory Factor Analysis - performed on 679 participants recruited during the study 2 – showing good indices of goodness of fit. The psychometric properties of the I-CAMM indicate good internal consistency (Cronbach’s alpha = 0.79 for the factor “ Mindfulness Skills”) and a good convergent validity with the scale of the internalizing problems of the YSR (r = -0,515) and with experiential avoidance and fusion measured with AFQ (r = -0,703). The mean scores of the I- CAMM are distributed differently between males and females; males reported significantly higher scores of “ Mindfulness Skills” than females. I-CAMM is a valid and reliable measure that can be easily used both in research and in clinical practice.
For further information please do not hesitate to contact us:
arianna.ristallo@gmail.com
martaschweiger26@gmail.com
CAMM - Persian Validity
CAMM - Persian ValidityMohsenabadi, H. and Shabani, M.J. and Assarian, F. & Zanjani, Z. (2020). Psychometric properties of the child and adolescent mindfulness measure: A psychological measure of mindfulness in youth. Iranian Journal of Psychiatry and Behavioral Sciences, 14 (1). http://eprints.iums.ac.ir/23950/
CAMM - Portuguese Validation
CAMM - Portuguese ValidationCunha, M., Galhardo, A., & Pinto-Gouveia, J. (2013). Child and Adolescent Mindfulness Measure (CAMM): Psychometric properties of the Portuguese version. Psicologia: Reflexão e Crítica, 26, 459-468. http://doi.org/10.1590/S0102-79722013000300005
CAMM - Spanish
CAMM - SpanishGuerra, J., García-Gómez, M., Turanzas, J., Cordón, J.R., Suárez-Jurado, C., & Mestre, J.M. (2019). A Brief Spanish Version of the Child and Adolescent Mindfulness Measure (CAMM). A Dispositional Mindfulness Measure. International Journal of Environmental Research and Public Health, 16(8), 1355. https://doi.org/10.3390/ijerph16081355 The CAMM Spanish Translation is in Appendix A.
García-Rubio, C., Rodríguez-Carvajal, R., Langer, A. I., Paniagua, D., Steinebach, P., Andreu, C. I., Vara, M. D., & Cebolla, A. (2019). Validation of the Spanish Version of the Child and Adolescent Mindfulness Measure (CAMM) with Samples of Spanish and Chilean Children and Adolescents. Mindfulness, 10(8), 1502–1517. https://doi.org/10.1007/s12671-019-01108-8
Gustin-García, M. G., & Alegre-Bravo, A. A. (2021). Validación de Child and Adolescent Mindfulness Measure en escolares de Lima, Perú. Revista Evaluar, 21(2), 63–79. https://doi.org/10.35670/1667-4545.v21.n2.34398
CAMM - Turkish
CAMM - TurkishZeynep Aydin Sünbül (2018). Psychometric Evaluation of Child and Adolescent Mindfulness Measure (CAMM) with Turkish Sample. International Journal of Education and Psychological Research (IJEPR), 7(2), 56-59.
The CAMM Turkish translation is here.
Children's Psychological Flexibility Questionnaire (CPFQ)
Children's Psychological Flexibility Questionnaire (CPFQ)References:
Lenoir, C., Hinman, J.M., Yi, Z. et al. (2022). Further Examination of the Children’s Psychological Flexibility Questionnaire (CPFQ): Convergent Validity and Age Appropriateness. Advances in Neurodevelopmental Disorders, 6, 224–233. https://doi.org/10.1007/s41252-022-00259-5
Bachmann, K., Hinman, J.M., Yi, Z. et al. (2021). Evaluating the Convergent and Divergent Validity of the Children’s Psychological Flexibility Questionnaire (CPFQ) among Children with Autism. Advances in Neurodevelopmental Disorders, 5, 298–303. https://doi.org/10.1007/s41252-021-00206-w
Dixon, M. R., & Paliliunas, D. (2018). Children’s psychological flexibility questionnaire. In Accept. Identify. Move. A Behavior Analytic Curriculum for Social-Emotional Development in Children (pp. 263-268). Carbondale, IL: Shawnee Scientific Press.
Chronic Pain Acceptance Questionnaire for Adolescents (CPAQ-A)
Chronic Pain Acceptance Questionnaire for Adolescents (CPAQ-A)Chronic Pain Acceptance Questionnaire for Adolescents (CPAQ-A)
- Shannon Connolly, Nuno Ferreira, Leona McGarrigle, & Leyla DeAmicis (2019). Further validation of the Chronic Pain Acceptance Questionnaire for Adolescents in a broader paediatric context. Journal of Contextual Behavioral Science, 12, 314-321. https://doi.org/10.1016/j.jcbs.2018.12.005
- Wallace, D. P., Harbeck-Weber, C., Whiteside, S. P., & Harrison, T. E. (2011). Adolescent acceptance of pain: confirmatory factor analysis and further validation of the chronic pain acceptance questionnaire, adolescent version. The journal of pain, 12(5), 591–599. https://doi.org/10.1016/j.jpain.2010.11.004
- McCracken, L.M., Gauntlett-Gilbert, J. & Eccleston, C. (2010). Acceptance of pain in adolescents with chronic pain: Validation of an adapted assessment instrument and preliminary correlation analyses. European Journal of Pain, 14, 316-320. https://doi.org/10.1016/j.ejpain.2009.05.002
Chronic Pain Acceptance Questionnaire, Parent Report (CPAQ-P)
- Simons, L. E., Sieberg, C. B., & Kaczynski, K. J. (2011). Measuring parent beliefs about child acceptance of pain: a preliminary validation of the Chronic Pain Acceptance Questionnaire, parent report. Pain, 152(10), 2294–2300. https://doi.org/10.1016/j.pain.2011.06.018
Diabetes Acceptance and Action Scale for Children and Adolescents (DAAS)
Diabetes Acceptance and Action Scale for Children and Adolescents (DAAS)The Diabetes Acceptance and Action Scale for Children and Adolescents is a 42-item measure that is being used to indicate levels of psychological flexibility in youth with Type 1 diabetes. (Authors: L. A. Greco & Hart 2005)
Scoring: To score the DAAS, first reverse score negatively worded items (see below), then sum all items. Higher scores on the DAAS should reflect higher levels of diabetes-related acceptance and action.
Reverse score key: 2, 4, 5, 6, 7, 8, 11, 13, 14, 17, 18, 19, 21, 22, 24, 25, 26, 27, 28, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42.
The authors are still in the process of collecting data. Preliminary data obtained thus far reveals statistically significant correlations: Diabetes-related quality of life = .36 (higher acceptance correlates with higher Quality of Life) Diabetes-related worry = -.41 Social anxiety = -.36 Adherence to medical regimen = .30"
Information quoted from Ciarrochi, J. & Bilich, L. (2006). Process measures of potential relevance to ACT. Unpublished manuscript, University of Wollongong, Australia.
References:
Berlin, KS, Keenan, ME, Cook, JL, et al. (2020). Measuring psychological flexibility in youth with type 1 diabetes. Pediatr Diabetes, 21, 1566–1574. https://doi.org/10.1111/pedi.13110
DAAS - Persian
DAAS - PersianRajaeiramsheh, F., Rezaie, Z., Davoudi, M. et al. (2021) Psychometric properties of the Persian versions of acceptance and action diabetes questionnaire (AADQ) and the diabetes acceptance and action scale (DAAS), in Iranian youth with type 1 diabetes. J Diabetes Metab Disord, 20, 655–663. https://doi.org/10.1007/s40200-021-00796-1 The DAAS Persian Translation is in the article's Supplementary Information.
Mindfulness Attention Awareness Scale in adolescent (MAAS-A)
Mindfulness Attention Awareness Scale in adolescent (MAAS-A)Brown, K. W., West, A. M., Loverich, T. M., & Biegel, G. M. (2011). Assessing adolescent mindfulness: Validation of an Adapted Mindful Attention Awareness Scale in adolescent normative and psychiatric populations. Psychological Assessment, 23(4), 1023–1033. https://doi.org/10.1037/a0021338
Goodman, M.S., Madni, L.A. & Semple, R.J. (2017). Measuring Mindfulness in Youth: Review of Current Assessments, Challenges, and Future Directions. Mindfulness, 8, 1409–1420. https://doi.org/10.1007/s12671-017-0719-9
MAAS-A - Chinese
MAAS-A - ChineseBlack, D. S., Sussman, S., Johnson, C. A., & Milam, J. (2012). Psychometric Assessment of the Mindful Attention Awareness Scale (MAAS) Among Chinese Adolescents. Assessment, 19(1), 42–52. https://doi.org/10.1177/1073191111415365
MAAS-A - Dutch
MAAS-A - Dutchde Bruin, E.I., Zijlstra, B.J.H., van de Weijer-Bergsma, E. et al. (2011) The Mindful Attention Awareness Scale for Adolescents (MAAS-A): Psychometric Properties in a Dutch Sample. Mindfulness, 2, 201–211. https://doi.org/10.1007/s12671-011-0061-6
MAAS-A - Italian
MAAS-A - ItalianMindfulness Attention Awareness Scale - Adolescent (Day to Day Experiences)
Brown, K. W., West, A. M., Loverich, T. M., & Biegel, G. M. (2011). Assessing adolescent mindfulness: Validation of an adapted Mindfulness
Attention Awareness Scale in adolescent normative and psychiatric populations. Psychological Assessment, 23, 1023–1033.
Referenza bibliografica: Rossi, E., Melchiorri, E., Panzera., A., Ristè, N., Carloni, V., Romitelli M. (2015). Validation study of the Italian version of the Mindfulness Attention Awareness Scale for Adolescents (MAAS-A). Poster presented at ACBS World Conference 13 Poster Session – Berlin, German- July 14-19, 2015.
Il presente studio è in corso di aggiornamento.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
MAAS-A - Norwegian
MAAS-A - NorwegianSmith, O. R. F., Melkevik, O., Samdal, O., Larsen, T. M., & Haug, E. (2017). Psychometric properties of the five-item version of the Mindful Awareness Attention Scale (MAAS) in Norwegian adolescents. Scandinavian Journal of Public Health, 45(4), 373–380. https://doi.org/10.1177/1403494817699321
MAAS-A - Persian
MAAS-A - PersianMohsenabadi, H. and Shabani, M.J. and Zanjani, Z. (2019) Factor structure and reliability of the mindfulness attention awareness scale for adolescents and the relationship between mindfulness and anxiety in adolescents. Iranian Journal of Psychiatry and Behavioral Sciences, 13 (1).
MAAS-A - Spanish
MAAS-A - SpanishCalvete, E., Sampedro, A., Orue, I. (2014) PROPIEDADES PSICOMÉTRICAS DE LA VERSIÓN ESPAÑOLA DE LA “ESCALA DE ATENCIÓN Y CONCIENCIA PLENA PARA ADOLESCENTES” (MINDFUL ATTENTION AWARENESS SCALE for ADOLESCENTS) (MAAS-A). Behavioral Psychology / Psicología Conductual, 22(2), 277-291
MAAS-A - Turkish
MAAS-A - TurkishTuran, M . (2020). Bilinçli Farkındalık Ölçeği Ergen Formu’nun Geçerlik ve Güvenirlik Çalışması. OPUS Uluslararası Toplum Araştırmaları Dergisi, Eğitim ve Toplum Özel sayısı, Cilt 16, 5608 - 5625. http://doi.org/10.26466/opus.683364
Parent Psychological Flexibility Questionnaire (PPFQ)
Parent Psychological Flexibility Questionnaire (PPFQ)McCracken, L.M. & Gauntlett-Gilbert, J. (2011) Role of psychological flexibility in parents of adolescents with chronic pain: Development of a measure and preliminary correlation analyses. Pain, 152, 780–785. https://doi.org/10.1016/j.pain.2010.12.001
Timmers, I, Simons, LE, Hernandez, JM, McCracken, LM, Wallace, DP. (2019) Parent psychological flexibility in the context of pediatric pain: Brief assessment and associations with parent behaviour and child functioning. Eur J Pain, 23, 1340– 1350. https://doi.org/10.1002/ejp.1403 The PPFQ-10 is attached to the article as supporting information.
PPFQ - Chinese
PPFQ - ChineseLI, Z., YANG, L., ZHU, L., & ZHU, Z. (2018) A preliminary study of validity and reliability of the Chinese version of the Parental Psychological Flexibility Questionnaire. Chinese Mental Health Journal, 32(2), 166-173. DOI: 10.3969/j.issn.1000-6729.2018.02.014
PPFQ - Swedish
PPFQ - SwedishWiwe Lipsker, C., Kanstrup, M., Holmström, L., Kemani, M., & Wicksell, R. K. (2016). The Parent Psychological Flexibility Questionnaire (PPFQ): Item Reduction and Validation in a Clinical Sample of Swedish Parents of Children with Chronic Pain. Children (Basel, Switzerland), 3(4), 32. https://doi.org/10.3390/children3040032
Parental Acceptance Questionnaire (6-PAQ)
Parental Acceptance Questionnaire (6-PAQ)Greene, R. L., Field, C. E., Fargo, J. D., & Twohig, M. P. (2015). Development and validation of the parental acceptance questionnaire (6-PAQ). Journal of Contextual Behavioral Science, 4(3), 170-175.
Abstract
The purpose of this study was to develop the Parental Acceptance Questionnaire (6-PAQ), an instrument measuring the six primary processes theorized to contribute to psychological flexibility among parents. Items were collaboratively developed by a team of experts. Parents (N=181) were recruited from a public elementary school and administered a pilot version of the 6-PAQ, which was refined using psychometric modeling procedures. The final version of the instrument yielded an overall internal consistency reliability coefficient of 0.84 with an average of 0.73 across the six psychological flexibility processes subscales. Results of a confirmatory factor analysis using items from the final version of the 6-PAQ suggested the measurement structure possessed an exceptional overall fit to the data: CFI=0.97, TLI=0.96, RMSEA=0.06 (90% confidence interval=0.05–0.08), and WRMR=0.86. Collectively, these results provide preliminary support for the 6-PAQ as a reliable and valid measure to assess parental psychological flexibility. Empirical and clinical implications of results as well as limitations and future directions are discussed.
Scoring:
The final version of the 6-PAQ is presented in a usable form in the appendix. The measure is completed by one parent or guardian with reference to one child. Scoring involves reversing items 1, 2, 5, 7, 10, 15, and 18, and then summing all items for the total score. Lower scores represent greater parental psychological flexibility whereas higher scores represent greater psychological inflexibility. The subscales are scored as follow: acceptance=items 3, 12, 14; defusion=6, 11, 16; being present=1, 8, 17; self as context=4, 9, 13; values=5, 10, 18; and committed action=2, 7, 15. Clinical norms and cutoffs are not yet available.
The 6-PAQ can be downloaded from the Utah State University ACT Research Group.
6-PAQ - Japanese
6-PAQ - JapaneseTatsuto Yamada & Yasushi Fujii (2020). Reliability and Validity of the Japanese-Version Parental Acceptance Questionnaire (6-PAQ). Child & Family Behavior Therapy, 42(4), 258-267. http://doi.org/10.1080/07317107.2020.1809198
6-PAQ - Portuguese Version
6-PAQ - Portuguese VersionFonseca, A., Canavarro, M.C. & Moreira, H. (2020). Is parental psychological flexibility a (uni) dimensional construct? A bifactor analysis of the Portuguese version of the parental acceptance questionnaire (6-PAQ). Current Psychology. https://doi.org/10.1007/s12144-020-00991-y The 6-PAQ translation is in the article's supplementary material.
6-PAQ - Spanish Validation
6-PAQ - Spanish ValidationParental Acceptance Questionnaire (6-PAQ) Spanish Validation: Juan M. Flujas-Contreras, Azucena García-Palacios, Inmaculada Gómez (2020) Spanish validation of the Parental Acceptance Questionnaire (6-PAQ). International Journal of Clinical and Health Psychology, 20 (2), 163-172. https://doi.org/10.1016/j.ijchp.2020.03.002
6-PAQ - Swedish
6-PAQ - SwedishStrandberg, S. (2022). Föräldraskap och psykologisk flexibilitet: En studie om prediktorer för utbrändhet, lidande och subjektiv livskvalitet hos föräldrar med och utan barn med kroniska tillstånd. Thesis. Karlstads Universitet. The Swedish transaltion of the 6-PAQ is in the appendix.
PAQ - Korean Adaptation
PAQ - Korean AdaptationSeung-Min Kim(서울여자대학교), Kyung Park(서울여자대학교) (2017) Korean Adaptation of the Parental Acceptance Questionnaire(K-4-PAQ). THE KOREAN JOURNAL OF HEALTH PSYCHOLOGY, Vol.22 No.3, pages 531 - 549.
Parental Acceptance and Action Questionnaire (PAAQ)
Parental Acceptance and Action Questionnaire (PAAQ)The Parental Acceptance and Action Questionnaire (PAAQ) is a specific AAQ measure designed to assess experiential avoidance in the context of parenting.
References
Cheron, D.M., Ehrenreich, J.T. & Pincus, D.B. (2009). Assessment of parental experiential avoidance in a clinical sample of children with anxiety disorders. Child Psychiatry and Human Development, 40, 383-403. https://doi.org/10.1007/s10578-009-0135-z
Holmberg Bergman, T., Sandred, A., Lindstrom, T., Lappalainen, P., Ghaderi, A., & Hirvikoski, T. (2024). A psychometric evaluation of the parental acceptance and action questionnaire (PAAQ) in parents of children with and without disabilities. Journal of Contextual Behavioral Science, 32, 100757. https://doi.org/10.1016/j.jcbs.2024.100757
PAAQ - Japanese
PAAQ - JapaneseReferences:
Yuki, M. & Hiroshi, S. (2018). Development of the Japanese Version of the Parental Acceptance and Action Questionnaire: A Preliminary Study. 人文論究, 67(4), 45-56. https://ci.nii.ac.jp/naid/120006401913/en/
Mizusaki, Y. & Sato, H. (2018). Preliminary study on the preparation of the Japanese version of the Parental Acceptance and Action Questionnaire. Humanit Res of KGU, 67, 45–56.
OKAJIMA, J. & Okajima, I. (2023). Developing and validating the Japanese version of the Parental Acceptance and Action Questionnaire among parents with infants and toddlers. International Journal of Environmental Research and Public Health, 20(9), 5674. https://doi.org/10.3390/ijerph20095674
PAAQ - Portuguese
PAAQ - Portuguese Navega, A.C. & Cunha, M. (2018) Questionário de Aceitação e Ação para Pais: desenvolvimento da versão portuguesa, estudo da estrutura fatorial e propriedades psicométricas. ISMT, Dissertaion. The Portuguese PAAQ is in the Appendix.
PAAQ - Spanish
PAAQ - SpanishCorina Shumi WONG CHEN (2018) Estilos parentales y evitación experiencial en padres de niños con trastorno por déficit de atención con o sin hiperactividad. Universidad Nacional Mayor de San Marcos, Thesis. The Spanish PAAQ is in the Anexo.
PsyFlex-A
PsyFlex-ASoares, R., Cunha, M., Massano-Cardoso, I., & Galhardo, A. (2023). Assessing psychological flexibility in adolescents: Validation of PsyFlex-A . Portuguese Journal of Behavioral and Social Research, 9(1), 1–18. DOI: 10.31211/rpics.2023.9.1.284
PsyFlex-A - Portuguese Version
PsyFlex-A - Portuguese VersionSoares, R., Cunha, M., Massano-Cardoso, I., & Galhardo, A. (2023). Assessing psychological flexibility in adolescents: Validation of PsyFlex-A . Portuguese Journal of Behavioral and Social Research, 9(1), 1–18. DOI: 10.31211/rpics.2023.9.1.284
Emotion Regulation Measures
Emotion Regulation Measures CommunityAffective Style Questionnaire (ASQ)
Affective Style Questionnaire (ASQ)ASQ: Hofmann, S.G. & Kashdan, T.B. (2010) The affective style questionnaire: Development and psychometric properties. Journal of Psychopathology and Behavioral Assessment, 32 (2), 255-263. http://doi.org/10.1007/s10862-009-9142-4 The Affective Style Questionnaire is in the Appendix.
ASQ for Youth (ASQ-y): Graser, J., Heimlich, C., Kelava, A., Hofmann, S.G., Stangier, U. & Schreiber, S. (2019). Erfassung der Emotionsregulation bei Jugendlichen anhand des Affective Style Questionnaire – Youth (ASQ-Y). Diagnostica, 65, 49-59. https://doi.org/10.1026/0012-1924/a000210 The ASQ-Y Translation is in the article's supplemental material.
ASQ - Chinese Version
ASQ - Chinese VersionWang, J., Xu, W., Fu, Z., Yu, W., He, L., Sun, L., He, J., & Hofmann, S. G. (2019). Psychometric properties of the Chinese version of the Affective Style Questionnaire and its role as a moderator of the relationship between stress and negative affect. Journal of Health Psychology, 24(5), 613–622. https://doi.org/10.1177/1359105316679722
ASQ - Dutch Translation
ASQ - Dutch TranslationErreygers, S., & Spooren, P. (2017). Factor Structure of the Affective Style Questionnaire in Flemish Adolescents. Psychologica Belgica, 57(2), 112–122. https://doi.org/10.5334/pb.369 The ASQ Dutch translation is in the Appendix.
ASQ - French Version
ASQ - French VersionMakowski, D., Sperduti, M., Lavallée, S. et al. (2020) Adaptation and Validation of a Short French Version of the Affective Style Questionnaire. J Cogn Ther,13, 146–158. https://doi.org/10.1007/s41811-019-00060-8
ASQ - German
ASQ - GermanGraser, J., Bohn, C., Kelava, A., Schreiber, F., Hofmann, S.G, and Stangier, U. (2012). Der „Affective Style Questionnaire (ASQ)”: Deutsche Adaption und Validitäten. Diagnostica, 58(2), 100-111. https://doi.org/10.1026/0012-1924/a000056
ASQ - Japanese
ASQ - JapaneseIto, M. & Hofmann, S.G. (2014) Culture and affect: the factor structure of the affective style questionnaire and its relation with depression and anxiety among Japanese. BMC Res Notes, 7, 590. https://doi.org/10.1186/1756-0500-7-590
ASQ - Korean
ASQ - Korean하정민, 조용래 (2015) Reliability and Validity of an Korean Version of the Affective Style Questionnaire. Korean Cognitive Behavioral Therapy, 15(2), 401 - 431.
ASQ - Swedish
ASQ - SwedishCecilia Tunberger (2011) Översättning och validering av Affective Style Questionnaire och samband med depression och ångest. Retrieved from https://lup.lub.lu.se/luur/download?func=downloadFile&recordOId=2026867&fileOId=2026868
The Swedish ASQ is at the end of the document.
ASQ - Turkish
ASQ - TurkishÖz Soysal, F. & Bakalım, O. (2021). Duygu Stilleri Anketi’nin Beliren Yetişkinlik Dönemindeki Bireylerde Geçerlik ve Güvenirlik Çalışması. Yükseköğretim ve Bilim Dergisi, 11(1) , 49-55 . Retrieved from https://dergipark.org.tr/en/pub/higheredusci/issue/62177/909406
ASQ-Y - German Version
ASQ-Y - German VersionGraser, J., Heimlich, C., Kelava, A., Hofmann, S.G., Stangier, U. & Schreiber, S. (2019). Erfassung der Emotionsregulation bei Jugendlichen anhand des Affective Style Questionnaire – Youth (ASQ-Y). Diagnostica, 65, 49-59. https://doi.org/10.1026/0012-1924/a000210 The ASQ-Y Translation is in the article's supplemental material.
Difficulties in Emotion Regulation Scale (DERS)
Difficulties in Emotion Regulation Scale (DERS)Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41-54. https://link.springer.com/article/10.1023/B:JOBA.0000007455.08539.94
Kaufman, E. A., Xia, M., Fosco, G., Yaptangco, M., Skidmore, C. R., & Crowell, S. (2016). The Difficulties in Emotion Regulation Scale Short Form (DERS-SF): validation and replication in adolescent and adult samples. Journal of Psychopathology and Behavioral Assessment, 38(443). https://doi.org/10.1007/s10862-015-9529-3 The English and Spanish versions of the DERS-SF can be found on miami.edu.
Skutch, J. M., Wang, S. B., Buqo, T., et al. (2019). Which Brief Is Best? Clarifying the Use of Three Brief Versions of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment, 41, 485–494. https://doi.org/10.1007/s10862-019-09736-z
DERS - Chinese
DERS - ChineseLi, J., Han, Z. R., Gao, M. M., Sun, X., & Ahemaitijiang, N. (2018). Psychometric properties of the Chinese version of the Difficulties in Emotion Regulation Scale (DERS): Factor structure, reliability, and validity. Psychological Assessment, 30(5), e1–e9. https://doi.org/10.1037/pas0000582
Zhao, Y., Wu, K., Wang, Y. et al. (2021) Construct validity of brief difficulties in emotion regulation scale and its revised version: evidence for a general factor. Curr Psychol. https://doi.org/10.1007/s12144-021-02056-0
DERS - Czech
DERS - CzechBenda, J. (2017) The Difficulties in Emotion Regulation Scale Short Form: a pilot study of the Czech version. E-psychologie, Electronic Journal of CMPS, 11(1). Retrieved from https://www.e-psycholog.eu/article/279
The Czech translation of the DERS-SF items is in table 3.
DERS - Finnish
DERS - FinnishWesterlund, M. & Santtila, P. (2018) A Finnish adaptation of the emotion regulation questionnaire (ERQ) and the difficulties in emotion regulation scale (DERS-16). Nordic Psychology, 70(4), 304-323. http://doi.org/10.1080/19012276.2018.1443279
Sami J. Eloranta, Riittakerttu Kaltiala, Nina Lindberg, Matti Kaivosoja & Kirsi Peltonen (2020) Validating measurement tools for mentalization, emotion regulation difficulties and identity diffusion among Finnish adolescents. Nordic Psychology. http://doi.org/10.1080/19012276.2020.1863852
DERS - French
DERS - FrenchGuylaine Côté, Patrick Gosselin, Isabel Dagenais (2013) Évaluation multidimensionnelle de la régulation des émotions : propriétés psychométriques d’une version francophone du Difficulties in Emotion Regulation Scale [Psychometric properties of a French version of the Difficulties in Emotion Regulation Scale]. Journal de Thérapie Comportementale et Cognitive, 23(2), 63-72. https://doi.org/10.1016/j.jtcc.2013.01.005
Dan-Glauser, E. S., & Scherer, K. R. (2013). The Difficulties in Emotion Regulation Scale (DERS): Factor structure and consistency of a French translation. Swiss Journal of Psychology, 72(1), 5–11. https://doi.org/10.1024/1421-0185/a000093
DERS - German
DERS - GermanRaphael Gutzweiler and Tina In-Albon (2018) Überprüfung der Gütekriterien der deutschen Version der Difficulties in Emotion Regulation Scale in einer klinischen und einer Schülerstichprobe Jugendlicher. Zeitschrift für Klinische Psychologie und Psychotherapie, 47(4), 274-286. https://doi.org/10.1026/1616-3443/a000506
Ehring, T., Svaldi, J., Tuschen-Caffier, B., & Berking, M. (2013) Validierung der Difficulties in Emotion Regulation Scale–deutsche Version. Manuskript. Universität Münster.
DERS - Greek
DERS - GreekKoushiou, M., & Karekla, M. (2016). Eating disorder risk: The role of sensitivity to negative affect and body-image inflexibility (Doctoral dissertation, University of Cyprus, Nicosia, Cyprus). Retrieved from https://gnosis.library.ucy.ac.cy/handle/7/39530
The Difficulties in Emotion Regulation Scale (DERS) Greek Translation is in Appendix B.
Mitsopoulou, E., Kafetsios, K., Karademas, E. et al. (2013) The Greek Version of the Difficulties in Emotion Regulation Scale: Testing the Factor Structure, Reliability and Validity in an Adult Community Sample. Journal of Psychopathology and Behavioral Assessment, 35, 123–131. https://doi.org/10.1007/s10862-012-9321-6
DERS - Gujarati
DERS - GujaratiSnow, N., Ward, R., Becker, S. & Raval, V. (2013). Measurement Invariance of the Difficulties in Emotion Regulation Scale in India and the United States. Journal of Educational and Developmental Psychology, 3(1), 147-157. http://dx.doi.org/10.5539/jedp.v3n1p147
DERS - Hebrew
DERS - HebrewReferences:
Segal, A. & Golan, M. (2016). Differences in emotion regulation along the eating disorder spectrum: Cross sectional study in adolescents out patient care. Journal of Psychology & Clinical Psychiatry, 6(1), 00314. DOI: 10.15406/jpcpy.2016.06.00314
Reuveni, I., Dan, R., Segman, R. et al. (2016). Emotional regulation difficulties and premenstrual symptoms among Israeli students. Archives of Women's Mental Health, 19, 1063–1070. Doi: 10.1007/s00737-016-0656-y
DERS - Hindi
DERS - HindiBhatnagar Prachi, Shukla Meenakshi, & Pandey Rakesh (2020) Validating the Factor Structure of the Hindi Version of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment, 42(2), 377-396. http://doi.org/10.1007/s10862-020-09796-6
DERS - Italian
DERS - ItalianGiromini, L., Velotti, P., de Campora, G., Bonalume, L. & Cesare Zavattini, G. (2012). Cultural Adaptation of the Difficulties in Emotion Regulation Scale: Reliability and Validity of an Italian Version. J. Clin. Psychol., 68, 989-1007. https://doi.org/10.1002/jclp.21876
Sighinolfi, C., Norcini Pala, A., Chiri, L. R., Marchetti, I., & Sica, C. (2010). Difficulties in emotion regulation scale (DERS): the italian translation and adaptation. PSICOTERAPIA COGNITIVA COMPORTAMENTALE, 16(2), 141–170. http://hdl.handle.net/1854/LU-1148235
DERS - Japanese
DERS - JapaneseKeiji TAKATA, Yoshitake TAKEBAYASHI, Keisuke TANAKA, Ayame TAMURA, Yoshinori SUGIURA (2013) The convergent validity of Japanese version of the Difficulties in Emotion Regulation Scale (DERS). The Proceedings of the Annual Convention of the Japanese Psychological Association, Volume 77, The 77th Annual Convention of the Japanese Psychological Association, Session ID 2EV-038, Pages 2EV-038. https://doi.org/10.4992/pacjpa.77.0_2EV-038
DERS - Korean
DERS - KoreanCho, Y., & Hong, S. (2013). The new factor structure of the Korean Version of the Difficulties in Emotion Regulation Scale (K-DERS) incorporating method factor. Measurement and Evaluation in Counseling and Development, 46(3), 192–201. https://doi.org/10.1177/0748175613484033
조용래 (2007) 정서조절곤란의 평가 한국판 척도의 심리측정적 속성 [Assessing Emotion Dysregulation: Psychometric Properties of the Korean Version of the Difficulties in Emotion Regulation Scale.] Korean Journal of Clinical Psychology, 26(4), 1015 - 1038.
DERS - Lithuanian
DERS - LithuanianŠeibokaitė, L., Endriulaitienė, A., Sullman, M. J., Markšaitytė, R., & Žardeckaitė-Matulaitienė, K. (2017). Difficulties in emotion regulation and risky driving among Lithuanian drivers. Traffic Injury Prevention, 18, 688-693. https://doi.org/10.1080/ 15389588.2017.1315109
DERS - Norwegian
DERS - NorwegianEndre Visted, Lin Sørensen, Berge Osnes, Julie L. Svendsen, Per-Einar Binder, & Elisabeth Schanche (2017) The Association between Self-Reported Difficulties in Emotion Regulation and Heart Rate Variability: The Salient Role of Not Accepting Negative Emotions. Front Psychol. https://doi.org/10.3389/fpsyg.2017.00328
DERS - Persian
DERS - PersianShahabi, M., Hasani, J., & Bjureberg, J. (2020). Psychometric Properties of the Brief Persian Version of the Difficulties in Emotion Regulation Scale (The DERS-16). Assessment for Effective Intervention, 45(2), 135–143. https://doi.org/10.1177/1534508418800210
kermani mamazandi, Z., Tale Pasand, S. (2018). Psychometric Characteristics of Difficulties in Emotion Regulation Scale in Semnan University Students. Journal of Instruction and Evaluation, 11(42), 117-142.
Mazaheri M. (2015). Psychometric Properties of the Persian Version of the Difficulties in Emotion Regulation Scale) DERS-6 & DERS-5- Revised (in an Iranian Clinical Sample. Iranian journal of psychiatry, 10(2), 115–122.
DERS - Portuguese
DERS - PortugueseCancian, A.C.M. et al. (2019) Psychometric properties of the Brazilian version of the Difficulties in Emotion Regulation Scale (DERS). Trends in Psychiatry and Psychotherapy, 41(01), 18-26. https://doi.org/10.1590/2237-6089-2017-0128
Miguel, F.K., Giromini, L., Colombarolli, M.S., Zuanazzi, A.C., & Zennaro, A. (2017). A Brazilian Investigation of the 36- and 16-Item Difficulties in Emotion Regulation Scales. J. Clin. Psychol., 73, 1146-1159. https://doi.org/10.1002/jclp.22404
Coutinhom, J. et al. (2010) Versão portuguesa da escala de dificuldades de regulação emocional e sua relação com sintomas psicopatológicos. Archives of Clinical Psychiatry (São Paulo), 37 (4). https://doi.org/10.1590/S0101-60832010000400001
DERS - Romanian
DERS - RomanianBostan, M.C. & Zaharia, D.V. (2016). Emotional dysregulation – factor structure and consistency in the Romanian version of the Difficulties in Emotion Regulation Scale (DERS). Analele Ştiinţifice ale Universităţii, Alexandru Ioan Cuza, din Iaşi. Psihologie, 2, 57-77.
DERS - Spanish
DERS - SpanishHervas, G., & Jodar, R. (2008). Adaptacion al castellano de la Escala de Dificultades en la Regulacion Emocional. Clınica y Salud, 19, 139156.
Isabel Gómez-Simón, Eva Penelo & Nuria de la Osa (2014) Factor structure and measurement invariance of the Difficulties Emotion Regulation Scale (DERS) in Spanish adolescents. Psicothema, 26(3), 401-408. https://doi.org/10.7334/psicothema2013.324 The Spanish translation is in Table 2.
Reivan-Ortiz, G. G., Rodas, P. E. O., & Reivan Ortiz, P. N. (2020). A Brief Version of the Difficulties in Emotion Regulation Scale (DERS): Validity Evidence in Ecuadorian Population. International Journal of Psychological Research, 13(2), 14–24. https://doi.org/10.21500/20112084.4325
Navarro, O., Restrepo-Ochoa, D., Rommel, D., Ghalaret, J-M., & Fleury-Bahi, G. (2021). Validation of a brief version of the Difficulties in Emotion Regulation Scale with a Spanish speaking population (DERS-S SF). Revista CES Psicología, 14(2), 71-88. https://doi.org/10.21615/cesp.5360
The Spanish translation of the Difficulties Emotion Regulation Scale-Short Form (DERS-SF) can be found at miami.edu.
DERS - Swedish
DERS - SwedishOlsson, S. (2010). Difficulties in Emotion Regulation Scale -ett instrument för att undersöka svårigheter med känsloreglering vid Borderline personlighetsstörning. Thesis: Stockholms Universitet/University of Stockholm. Retrieved from https://www.diva-portal.org/smash/record.jsf?dswid=7400&pid=diva2%3A325427
The DERS Swedish Version is in the Appendix.
DERS - Turkish
DERS - TurkishYiğit, İ. &Guzey Yiğit, M. (2019). Psychometric Properties of Turkish Version of Difficulties in Emotion Regulation Scale-Brief Form (DERS-16). Current Psychology, 38, 1503–1511. https://doi.org/10.1007/s12144-017-9712-7
Rugancı, R.N. & Gençöz, T. (2010). Psychometric properties of a Turkish version of the difficulties in emotion regulation scale. Journal of Clinical Psychology, 66, 442-455. https://doi.org/10.1002/jclp.20665
DERS - Urdu
DERS - UrduZafar, H., Debowska, A., & Boduszek, D. (2021). Emotion regulation difficulties and psychopathology among Pakistani adolescents. Clinical Child Psychology and Psychiatry, 26(1), 121–139. https://doi.org/10.1177/1359104520969765
State Difficulties in Emotion Regulation Scale (S-DERS)
State Difficulties in Emotion Regulation Scale (S-DERS)Lavender, J.M, Tull, M.T., DiLillo, D., Messman-Moore, T., & Gratz, K.L. (2017). Development and validation of a state-based measure of emotion dysregulation: The State Difficulties in Emotion Regulation Scale (S-DERS). Assessment, 24 (2), 197-209. https://doi.org/10.1177/1073191115601218
Emotion Efficacy Scale
Emotion Efficacy Scale adminFusion Measures
Fusion MeasuresCognitive Fusion Questionnaire (CFQ)
Cognitive Fusion Questionnaire (CFQ)CFQ Update 12th September 2022
The Cognitive Fusion Questionnaire is a brief self report measure of cognitive fusion. It is now in print at Behavior Therapy and can be cited as follows:
Gillanders, D. T., Bolderston, H., Bond, F. W., Dempster, M., Flaxman, P. E., Campbell, L., Kerr, S., Tansey, L., Noel, P., Ferenbach, C., Masley, S., Roach, L., Lloyd, J., May, L., Clarke, S., Remington, R. (2014) The development and initial validation of The Cognitive Fusion Questionnaire. Behavior Therapy, 45, 83-101, DOI: 10.1016/j.beth.2013.09.001
We have been working on the development of this measure since 2007 and the process of scale construction and psychometric properties are described in the attached manuscript. The CFQ is free to use for clinical and research purposes, permission is not needed. A number of people have made translations of the CFQ into other languages and we ask them to make sub pages to this page, sharing the measure and any psychometric properties. If you wish to translate the CFQ into a non English language, please do contact David Gillanders, to ensure a translation has not already been made. To our knowledge there are currently translations in Dutch, French, Spanish, German, Portuguese (European and Braziliian), Japanese, Hebrew, Farsi, Greek, Turkish, Catalan, Polish, Italian, Chinese, Korean, Romanian, Swedish, and Arabic.
The final manuscript can be accessed here: http://dx.doi.org/10.1016/j.beth.2013.09.001
We hope this measure is useful to the development of ACT and contextual science across diverse fields, please do use it.
David Gillanders, University of Edinburgh, Helen Bolderston, Southampton University & Frank Bond, University of London, Goldsmiths
Cognitive Fusion Questionnaire - Arabic Translation
Cognitive Fusion Questionnaire - Arabic TranslationThis Arabic translation of the CFQ has been conducted by Dr Hanan Alsofyani of King Khalid University, files attached are written in arabic. To contact Dr Alsofyani email him at doctorhanan2030@gmail.com
Cognitive Fusion Questionnaire - Catalan Translation adolescents sample
Cognitive Fusion Questionnaire - Catalan Translation adolescents sampleALGOS, a research on pain team, has translated CFQ into Catalan and validated it for adolescent population (11-20 years old). A paper with a description of the psychometric properties in a sample of adolescents has been published.
Solé, E., Racine, M., Castarlenas, E., Vega, R. de la, Tomé-Pires, C., Jensen, M., & Miró, J. (2015). The psychometric properties of the Cognitive Fusion Questionnaire in adolescents. European Journal of Psychological Assessment. https://doi.org/10.1027/1015-5759/a000244
If you need further information, you can contact algos.dolor@urv.cat or Ester Solé (ester.sole@urv.cat).
Cognitive Fusion Questionnaire - Chinese Validity
Cognitive Fusion Questionnaire - Chinese ValidityZHANG Wei-Chen, JI Yang, LI Xin, GUO Hui-Na, ZHU Zhuo-Hong (2014) Reliability and validity of the Chinese version of the Cognitive Fusion Questionnaire. Chinese Mental Health Journal, 2014, Issue 1, 40-44. Retrieved from China/Asia On Demand
Conclusion: CFQ-F中文版具有较好的信效度,可在我国用于认知融合相关研究. Conclusion: The Chinese version of CFQ-F has good reliability and validity and can be used for cognitive fusion related research in China.
王小龙, 曹静, 安静, 丁万兵, 索玉兰, 苏华, 李燕, 祝卓宏, 汤永隆 (2015). 中文接纳与行动问卷第二版(AAQ-II)与认知融合问卷(CFQ)在回族和哈萨克族青少年中的信效度检验. 心理学进展, 5(11), 695-701. [Wang Xiaolong, Cao Jing, Jing Jing, Ding Wanbing, Suo Yulan, Su Hua, Li Yan, Zhu Zhuohong, Tang Yonglong (2015). Chinese Acceptance and Action Questionnaire Second Edition (AAQ-II) and Cognitive Fusion Questionnaire (CFQ ) in Hui and Kazak adolescents. Advances in Psychology, 5(11) , 695-701.] http://dx.doi.org/10.12677/AP.2015.511090
赵雯倩,李小妹,王雯,李璐璐,张蒙悦. (2020). 中文版认知融合问卷在乳腺癌人群中的信效度研究 [Reliability and validity of Chinese version of cognitive fusion questionnaire in breast cancer patients]. Contemporary Nurse, 27(06):25-26.
Cognitive Fusion Questionnaire - Dutch Translation
Cognitive Fusion Questionnaire - Dutch TranslationDutch translation CFQ13 (September 2011)
The CFQ13 (developed by David Gillanders, Helen Bolderston & Frank Bond), has been translated into Dutch by Tim Batink and Hubert de Mey and is being researched for its psychometric properties. The preliminary results of those studies are promising; the internal validity looks good as well as the correlations with corresponding questionnaires. We are planning to report more elaborate about our results, begin 2012.
The Dutch version of the CFQ13, with some basic information about the psychometric properties and two non-clinical samples is downloadable for ACBS-members.
Tim Batink, Maastricht University & Hubert de Mey, Radboud University
Cognitive Fusion Questionnaire - French Validation
Cognitive Fusion Questionnaire - French ValidationDionne, F., Gagnon, J., Balbinotti, M., Peixoto, E. M., Martel, M.-E., Gillanders, D., & Monestès, J.-L. (2016). "Buying into thoughts”: Validation of a French translation of the Cognitive Fusion Questionnaire. Canadian Journal of Behavioural Science / Revue canadienne des sciences du comportement, 48(4), 278–285. https://doi.org/10.1037/cbs0000053
Dionne, F., Balbinotti, M., Gillanders, D., Gagnon, J., & Monestès, J. L. (2014). Validation of the Cognitive Fusion Questionnaire in a French-speaking population. Poster presentation at ACBS Annual World Conference XII. Minneapolis, MN. The French Translations of the CFQ items are in the poster (See attachment below)
Cognitive Fusion Questionnaire - German Validation
Cognitive Fusion Questionnaire - German ValidationChina, C., Hansen, L.B., Gillanders, D.T., Benninghoven, D. (2018) Concept and validation of the German version of the Cognitive Fusion Questionnaire (CFQ-D). Journal of Contextual Behavioral Science, 9, 30-35. https://doi.org/10.1016/j.jcbs.2018.06.003 The German translation of the CFQ is in the Appendix.
Cognitive Fusion Questionnaire - Greek translation
Cognitive Fusion Questionnaire - Greek translationZachariaa, M. et al. (2021). Does Cognitive Fusion show up similarly across two behavioral health samples? Psychometric properties and invariance of the Greek–Cognitive Fusion Questionnaire (G-CFQ). Journal of Contextual Behavioral Science, 21, 212-221. https://doi.org/10.1016/j.jcbs.2021.01.003 The Greek CFQ items are in Table 2.
(Login to your ACBS account to see the attachments)
Cognitive Fusion Questionnaire - Italian version
Cognitive Fusion Questionnaire - Italian versionDonati, M. A., Berrocal, C., Bernini, O., Gori, C., & Primi, C. (2021). Measuring cognitive fusion through the Cognitive Fusion Questionnaire-7: Measurement invariance across non-clinical and clinical psychological samples. PloS one, 16(2), e0246434. https://doi.org/10.1371/journal.pone.0246434 The Italian translation of the CFQ-7 is in Appendix SI.
Oppo, A., Prevedini, A. B., Dell'Orco, F., Dordoni, P., Presti, G., Gillanders, D. T., & Moderato, P. (2019). Fusione e defusione. Adattamento e proprieta psicometriche della versione Italiana del Cognitive Fusion Questionnaire (I-CFQ) [Fusion and defusion. Adaptation and psychometric properties of the Italian version of the Cognitive Fusion Questionnaire (I-CFQ)]. Psicoterapia Cognitiva e Comportamentale, 25(1), 53–73.
Researchers from IESCUM, IULM University and ACT Italia are now working at the italian validation of CFQ. Preliminary data had been presented at ACBS Annual World Conference X in Washington DC in 2012 and at XVI AIAMC Conference in Pescara 2012.
Details of these studies can be seen here:
Dell’Orco F., Prevedini A., Oppo A., Presti, G.B., Moderato P.(2012). Validation study of the Italian version of the Cognitive Fusion Questionnaire (CFQ), poster presentation at ACBS Annual World Conference X Washington 22-25 luglio 2012
Dell’Orco F., Prevedini A., Oppo A., Presti, G.B., Moderato P.(2012). Studio di validazione italiana del Cognitive Fusion Questionnaire (CFQ), presentation in symposiun at XVI Congresso Associazione Italiana di Analisi e Modificazione del Comportamento - AIAMC, Pescara 25-28 Ottobre 2012.
For any further information, please write to: francesco.dellorco@iulm.it or annaprevedini@gmail.com
CFQ-13 Italian
CFQ-13 ItalianCognitive Fusion Questionnaire (CFQ-13)
David T. Gillanders, Helen Bolderston, Frank W. Bond, Maria Dempster, Paul E. Flaxman, Lindsey Campbell, Sian Kerr, Louise Tansey, Penelope Noel, Clive Ferenbach, Samantha Masley, Louise Roach, Joda Lloyd, Lauraine Mann, Susan Clarke, Bob Remington, The development and initial validation of The Cognitive Fusion Questionnaire, Behavior Therapy, Available online 18 September 2013, ISSN 0005-7894, http://dx.doi.org/10.1016/j.beth.2013.09.001.
Traduzione Italiana (1.0) a cura di Violini, P., Ristè, N., Melchiorri, E., Cioci, M., Rossi, E., Francesconi, C. (2013) AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (2.0) a cura di Violini, P., Ristè, N., Melchiorri, E., Cioci, M., Rossi, E., Francesconi, C., Lijoi, E. (2013) AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (3.0) a cura di Violini, P., Ristè, N., Lijoi, E., Melchiorri, E., Rossi, E., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Ristè, N., Lijoi, E., Rossi, E., Violini, P., Melchiorri, E., Panzera, A., (2014). A preliminary study of the Cognitive Fusion Questionnaire (CFQ) in Italian adolescents. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014
Per informazioni: segreteria@aiscc.it – www.aiscc.it
Cognitive Fusion Questionnaire - Japanese Validation
Cognitive Fusion Questionnaire - Japanese ValidationTaiki Shima et al (2016) Examining the validity of the revised Cognitive Fusion Questionnaire 13-item and 7-item editions. Japanese Journal of Behavior Therapy, 42(1), 73-83. https://doi.org/10.24468/jjbt.42.1_73 The CFQ Japanese Translation is in the Appendix.
Kang, R.N., Tanaka, Y., Sato, T., Maeda, S. & Shimada, H. (2023 in press). The Development of a Japanese Version of the State Cognitive Fusion Questionnaire. Japanese Psychological Research. https://doi.org/10.1111/jpr.12453
Cognitive Fusion Questionnaire - Korean Version
Cognitive Fusion Questionnaire - Korean VersionKim, B. & Cho, S. (2015). Psychometric properties of a Korean version of the cognitive fusion questionnaire. Social Behavior and Personality: International Journal, 43 (1), 1715-1724. https://doi.org//10.2224/sbp.2015.43.10.1715
Cognitive Fusion Questionnaire - Norwegian
Cognitive Fusion Questionnaire - NorwegianTom Østergaard, Tobias Lundgren, Robert D. Zettle, Nils Inge Landrø, & Vegard Øksendal Haaland (2020) Psychological Flexibility in Depression Relapse Prevention: Processes of Change and Positive Mental Health in Group-Based ACT for Residual Symptoms. Front. Psychol. https://doi.org/10.3389/fpsyg.2020.00528
Cognitive Fusion Questionnaire - PERSIAN/FARSI Translation
Cognitive Fusion Questionnaire - PERSIAN/FARSI Translation
Cognitive Fusion Questionnaire - PERSIAN/FARSI Translation
پرسشنامه ی فیوژن شناختی که به زبان فارسی ترجمه شده است
تشکر از استاد مهدی گنجی
Esmail Soltani, Sirous Momenzadeh, Zohreh Hoseini. Reliability and Validity of the Cognitive Fusion Questionnaire in Iran University Students.
Esmail Soltani, Sirous Momenzadeh, Zohreh Hoseini. Reliability and Validity of the Cognitive Fusion Questionnaire in Iran University Students.Soltani E, Momenzadeh S, Hoseini Z . Psychometric properties of the farsi Cognitive Fusion Questionnaire .Pejouhandeh. Under review. Text in persian.
email:ssoltani65@gmail.com
The purpose of the present study was to examine the validity and reliability of the Cognitive Fusion Questionnaire (CFQ) in Iranian university students. 324 university students from Shahid Beheshti University of medical sciences participated in the present study during the winter semester of the 2014- 2015 academic year. Factor analysis by principle component analysis method, convergent validity were conducted to examine the validity of the CFQ. To calculate the reliability of the CFQ, Cronbach alpha and test- retest reliability were used. Results from factor analysis by principle component analysis method yielded one factors that explained 54.89% of the variance.this result is confirmed by AMOS. Support for the convergent and discriminant validity of the CFQ via its positive correlations with the Believability of Anxious Feelings and Thoughts Questionnaire, Acceptance and Action Questionnaire – II, Social Interaction Anxiety Scale, and negative correlations with Social Anxiety - Acceptance and Action Questionnaire, Valued Living Questionnaire And WHOQOL- BREF was obtained. The reliability of the CFQ via calculating Cronbach’s alpha and test- retest coefficients were yielded 0.86 and 0.86, respectively.
Cognitive Fusion Questionnaire - Polish Version
Cognitive Fusion Questionnaire - Polish VersionThe Cognitive Fusion Questionnaire was translated into Polish in the spring of 2014 by Lidia Budziszewska, MSc, Universidad de Almeria, Spain; Stanislaw Malicki, MSc, Akershus University Hospital, Norway and Joanna Dudek, MSc, University of Social Sciences and Humanities, Poland.
The enclosed Polish translation, titled „Kwestionariusz Fuzji Poznawczej (KFP)”, is a consensus-version with an independent back-translation.
The Polish version of CFQ has yet to be validated, but it was already used in a cross-sectional study conducted by Stanislaw Malicki in 2014 on a mixed (clinical and non-clinical) sample of Polish adults (N=197). The Polish CFQ (KFP) was administered together with Polish versions of: Acceptance and Action Questionnaire - II (AAQ-II), Mindful Attention Awareness Scale (MAAS – Brown & Ryan), Self-Compassion Scale – Short Form (Neff), Fears of Compassion Scales (Gilbert), Early Memories of Warmth Scale (Gilbert), Early Life Events Scale (Gilbert) and Relationships Questionnaire (Bartholomew & Horowitz). A summary document with correlational data will be available here soon.
For further information contact: Stanislaw Malicki, Akershus University Hospital, Norway; email: stanislaw.malicki@ahus.no
CFQ: Baran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
See attachment CFQ Polish.
Cognitive Fusion Questionnaire - Portuguese
Cognitive Fusion Questionnaire - Portuguese CommunityCognitive Fusion Questionnaire (CFQ-7)_Brazilian Portuguese version
Cognitive Fusion Questionnaire (CFQ-7)_Brazilian Portuguese versionCFQ Brazilian Portuguese version is attached to this webpage.
Corresponding author: Paola Lucena-Santos, Ph.D. in Clinical Psychology.
E-mail: paolabc2.lucena@gmail.com
WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra).
References:
Lucena-Santos, P., Carvalho, S., Pinto-Gouveia, J., Gillanders, D., & Oliveira, M. S. (2017). Cognitive Fusion Questionnaire: Exploring measurement invariance across three groups of Brazilian women and the role of cognitive fusion as a mediator in the relationship between rumination and depression. Journal of Contextual Behavioral Science, 6(1): 53-62. http://dx.doi.org/10.1016/j.jcbs.2017.02.004
Pinto-Gouveia, J., Dinis, A., Gregório, S. et al. (2020). Concurrent effects of different psychological processes in the prediction of depressive symptoms – the role of cognitive fusion. Curr Psychol, 39, 528–539. https://doi.org/10.1007/s12144-017-9767-5
Cognitive Fusion Questionnaire (CFQ-7)_European Portuguese
Cognitive Fusion Questionnaire (CFQ-7)_European PortugueseContact person: Alexandra Dinis
E-mail: alexandra.m.b.dinis@gmail.com
Affiliation: CINEICC - Cognitive Behavioral Research Center
Faculty of Psychology and Education Sciences, University of Coimbra
Rua do Colégio Novo, Apartado 6153. 3001-802 Coimbra, Portugal.
Cognitive Fusion Questionnaire - Spanish Translation
Cognitive Fusion Questionnaire - Spanish TranslationA team from Madrid developed and published a Spanish translation of the CFQ. Details of these studies can be seen here:
Romero-Moreno, R., Máquez-González, M., Losada, A. et al. (2012). Reliability and validity of the Spanish version of the Cognitive Fusion Questionnaire in dementia caregivers. The Gerontologist, 52, 54-55.
Romero-Moreno, R., Márquez-González, M., Losada, A., Gillanders, D. T.. & Fernández- Fernández, V. (2014). Cognitive fusion in dementia caregiving: psychometric properties of the Spanish version of the Cognitive Fusion Questionnaire. Behavioral Psychology, 22, 1, 117-132.
Citations:
Ruiz, F.J., Suárez-Falcón, J.C., Cárdenas-Sierra, S. et al. (2016). Psychometric Properties of the Acceptance and Action Questionnaire–II in Colombia. Psychol Rec, 66, 429–437. https://doi.org/10.1007/s40732-016-0183-2
José Quintero, P.S., Rodríguez Biglieri, R., Etchezahar, & Gillanders, D. (2022). The Argentinian version of the cognitive fusion questionnaire: Psychometric properties and the role of cognitive fusion as a predictor of pathological worry. Curr Psychol, 41, 2546–2557. https://doi.org/10.1007/s12144-020-00767-4 The CFQ Argentinian version is in the appendix.
Logged in members can download the questionnaire and the validation article below.
Cognitive Fusion Questionnaire - Swedish
Cognitive Fusion Questionnaire - SwedishNilsson, P. (2021). Psykologisk Inflexibilitet och Kognitiv Fusion hos Vuxna med Autism, En Studie om Acceptance and Commitment Therapy. Thesis: Mittuniversitetet/Mid Sweden University. Retrived from http://www.diva-portal.org/smash/record.jsf?pid=diva2%3A1566478&dswid=1065
The CFQ-7 Swedish Version is in Appendix (Bilaga) 3.2.
Cognitive Fusion Questionnaire - Turkish Translation
Cognitive Fusion Questionnaire - Turkish TranslationKervancioglu, A., Aydin, . Y., Sakarya, . D., Duymaz, . G. & Ozdel, . K. (2023) ADAPTATION OF COGNITIVE FUSION QUESTIONNAIRE TO TURKISH: A VALIDITY AND RELIABILITY STUDY. Journal of Cognitive-Behavioral Psychotherapy and Research, 12 (1), 50-56. doi:10.5455/JCBPR.19971
Attached file with the name CFQ-turkish.pdf includes the Turkish version of the scale.
Cognitive Fusion Questionnaire - Urdu Translation
Cognitive Fusion Questionnaire - Urdu TranslationThe Urdu translation of the CFQ is downloadable for ACBS-members. Translation and Validation of Multidimensional Psychological Flexibility Inventory is in process.
Rabia Khawar, Ph.D - rabiakhawar@gcuf.edu.pk
Associate Professor
Chairperson Department of Applied Psychology
GC University Faisalabad
Cognitive Fusion Questionnaire - Body Image (CFQ-BI)
Cognitive Fusion Questionnaire - Body Image (CFQ-BI)Ferreira, C., Trindade, I. A., Duarte, C., & Pinto-Gouveia, J. (2015). Getting entangled with body image: Development and validation of a new measure. Psychology and Psychotherapy: Theory, Research and Practice, 88(3), 304–316. https://doi.org/10.1111/papt.12047 (original version in Portuguese from Portugal)
Barney, J.L. et al (2021) Confirmatory factor analysis and measurement invariance of the Cognitive Fusion Questionnaire-Body Image in a clinical eating disorder sample. Body Image, 38, 262-269. https://doi.org/10.1016/j.bodyim.2021.04.012
CFQ-BI - Brazilian Portuguese
CFQ-BI - Brazilian PortugueseCorresponding author: Paola Lucena-Santos, Ph.D. in Clinical Psychology.
E-mail: paolabc2.lucena@gmail.com
WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
Address: Rua do Colégio Novo, Apartado 6153. Postal Code: 3001-802. Coimbra, Portugal.
Reference:
Lucena-Santos, P., Trindade, I. A., Oliveira, M. S., & Pinto-Gouveia, J. (2017). Cognitive Fusion Questionnaire - Body Image: psychometric properties and its incremental power in the prediction of binge eating severity. The Journal of Psychology Interdisciplinary and Applied, doi: 10.1080/00223980.2017.1305322
Cognitive Fusion Questionnaire - Chronic Illness (CFQ-CI)
Cognitive Fusion Questionnaire - Chronic Illness (CFQ-CI)Trindade, I. A., Ferreira, C., & Pinto-Gouveia, J. (2018). Assessment of chronic illness-related cognitive fusion: Preliminary development and validation of a new scale with an IBD sample. Journal of Clinical Psychology in Medical Settings. doi: 10.1007/s10880-017-9536-5
(original version in Portuguese from Portugal)
CFQ-CI - Persian
CFQ-CI - PersianSoltani, E., Izadi, S., Sharifi, P., & Poursadeghfard, M. (2022). Psychometric Properties of the Persian Version of Cognitive Fusion Questionnaire-Chronic Illness in Multiple Sclerosis. Iranian Journal of Psychiatry and Behavioral Sciences, 16(1):e113524. DOI: 10.5812/ijpbs.113524.
CFQ-CI - Portuguese
CFQ-CI - PortugueseTrindade, I. A., Ferreira, C., & Pinto-Gouveia, J. (2018). Assessment of chronic illness-related cognitive fusion: Preliminary development and validation of a new scale with an IBD sample. Journal of Clinical Psychology in Medical Settings. doi: 10.1007/s10880-017-9536-5
(original version in Portuguese from Portugal)
Automatic Thoughts Questionnaire (ATQ)
Automatic Thoughts Questionnaire (ATQ)The Automatic Thoughts Questionnaire (ATQ; Hollon & Kendall, 1980). The ATQ measures depressogenic thought frequency. This measure is commonly used in depression studies examining the impact of cognitive therapy. However, the ATQ-B is a revision to this measure by Zettle and Hayes (ATQ-B, Zettle & Hayes, 1986) aimed at assessing the believability of these depressive thoughts if they occur and it has been used as a proxy measure for defusion in the ACT community. We recommend that you use both subscales; the ATQ-F for frequency of automatic/depressive thoughts and the ATQ-B for believability of (or fusion with) these thoughts. Scoring for the measure is typically a simple sum score for the F sub scale and the B sub scale. The F and B scores can be used in analyses as separate entities and have been shown to be differentially related to outcomes (e.g., frequency of thoughts was not reduced at post treatment but believability of them was reduced) in studies of depression using behavioral interventions.
Reference: Zettle, R. D. & Hayes, S. C. (1986). Dysfunctional control by client verbal behavior: The context of reason giving. The Analysis of Verbal Behavior, 4, 30 38.
ATQ - Portuguese
ATQ - PortuguesePereira, I., Matos, A., & Azevedo, A. (2014). Portuguese version of the Automatic Thoughts Questionnaire – Revised: Relation with depressive symptomatology in adolescents. Psicologia, Saúde & Doenças, 15, 37-47. http://doi.org/10.15309/14psd150105
ATQ - Chinese
ATQ - ChineseCAO Ri-fang, CHENG Shu-lin, TANG Wen-xin, SONG Hai-dong (2001) The Reliability and Validity of Automatic Thoughts Questionnaire. CHINESE JOURNAL OF CLINICAL PSYCHOLOGY, 2, 108.
Jia‐Yan Pan, Shengquan Ye, Petrus Ng (2015) Validation of the Automatic Thoughts Questionnaire (ATQ) Among Mainland Chinese Students in Hong Kong. Journal of Clinical Psychology, 72, 1, 38-48. DOI: 10.1002/jclp.22193
ATQ - Danish
ATQ - DanishLichtenstein, M.B. et al (2019). A psychometric evaluation of the automatic thoughts questionnaire in Danish adolescents and emerging adults. Nordic Psychology, 71(4), 262-275. http://doi.org/10.1080/19012276.2019.1604252
ATQ - Dutch
ATQ - DutchBoelen PA. (2007) Psychometric properties of the Dutch version of the Automatic Thoughts Questionnaire - Positive (ATQ - P). Cognitive Behaviour Therapy, 36(1), 23-33. http://doi.org/10.1080/16506070600874315
Raes, F., & Hermans, D. (2011). De Nederlandstalige versie van de Automatic Thoughts Questionnaire-Revised (ATQ-R-NL) [The Dutch version of the Automatic Thoughts Questionnaire-Revised (ATQ-R-NL)]. Gedragstherapie, 44(1), 53–62.
ATQ - French
ATQ - FrenchLebreuilly, R. & Alsaleh, M. (2019) Élaboration d’un questionnaire court de pensées automatiques positives et négatives (ATQ-18-Fr) auprès d’étudiants français [Study to develop the positive and negative Automatic Thoughts Questionnaire (ATQ-18-Fr) for French students]. Journal de Thérapie Comportementale et Cognitive, 29(3), 132-139. https://doi.org/10.1016/j.jtcc.2019.01.003
ATQ - Italian
ATQ - ItalianAutomatic Thoughts Questionnaire (ATQ)
Zettle, R. D. & Hayes, S. C. (1986). Dysfunctional control by client verbal behavior: The context of reason giving. The Analysis of Verbal Behavior, 4, 30-38.
Traduzione Italiana (1.0) a cura di Melchiorri, E., Francesconi, C., Rossi, E., Ristè, N., Violini, P., Cioci, M. (2013). AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (2.0) a cura di Melchiorri, E., Francesconi, C., Rossi, E., Ristè, N., Violini, P., Lijoi, E., Cioci, M. (2013) AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (3.0) a cura di Melchiorri, E., Rossi, E., Violini, P., Ristè, N., Lijoi, E., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Rossi, E., Melchiorri, E., Lijoi, E., Ristè, N., Violini, P., Panzera, A., (2014). A Preliminary Study on Validating the Automatic Thoughts Questionnaire (ATQ) in Italian Adolescents. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
ATQ - Japanese
ATQ - JapaneseTANAKA, N., UJI, M., HIRAMURA, H., CHEN, Z., SHIKAI, N. and KITAMURA, T. (2006). Cognitive patterns and depression: Study of a Japanese university student population. Psychiatry and Clinical Neurosciences, 60, 358-364. https://doi.org/10.1111/j.1440-1819.2006.01514.x
ATQ - Malay
ATQ - MalayOei, T. P. S.; Mukhtar, F. (2008) Exploratory and Confirmatory Factor Validation and Psychometric Properties of the automatic Thoughts Questionnaire for Malays (ATQ-Malay) in Malaysia. Hong Kong Journal of Psychiatry, 18(3), 92-100.
ATQ - Norwegian
ATQ - NorwegianChioqueta, A. & Stiles, T. (2004). Norwegian version of the Automatic Thoughts Questionnaire: A reliability and validity study. Cognitive Behaviour Therapy, 33, 79-82. http://doi.org/10.1080/16506070310016031
ATQ - Persian
ATQ - PersianGhassemzadeh, H., Mojtabai, R., Karamghadiri, N., & Ebrahimkhani, N. (2006). Psychometric properties of a Persian-language version of the Automatic Thoughts Questionnaire: ATQ-Persian. The International journal of social psychiatry, 52(2), 127–137. https://doi.org/10.1177/0020764006062095
ATQ - Spanish
ATQ - SpanishRuiz, F., Suárez-Falcón, J., & Riaño-Hernández, D. (2017). Validity Evidence of the Spanish Version of the Automatic Thoughts Questionnaire–8 in Colombia. The Spanish Journal of Psychology, 20, E12. http://doi.org/10.1017/sjp.2017.7
Ruiz, F.J., Segura-Vargas M.A., Odriozola-González, P., & Suárez-Falcón J.C. (2020). Psychometric properties of the Automatic Thoughts Questionnaire-8 in two Spanish nonclinical samples. PeerJ, 8,e9747 https://doi.org/10.7717/peerj.9747
ATQ - Tamil
ATQ - TamilDr. Veera Balaji Kumar has shared his Tamil translation of ATQ. Therapists working with Tamil speaking clients can utilize this measure.
Proviso: Although this translation was cross-checked by a language expert and found workable in Veera's practice, it has not been psychometrically tested for accuracy.
ATQ - Turkish
ATQ - TurkishBozkurt, N , Aysan, F . (2013). GELİŞTİRİLMİŞ OTOMATİK DÜŞÜNCELER ÖLÇEĞI(ODÖ - G)'NİN LİSE ÖĞRENCİLERİ İÇİN GEÇERLİK VE GÜVENİRLİK ÇALIŞMASI . Marmara Üniversitesi Atatürk Eğitim Fakültesi Eğitim Bilimleri Dergisi , 12 (12) , 91-108 .
Believability of Anxious Feelings and Thoughts Questionnaire (BAFT)
Believability of Anxious Feelings and Thoughts Questionnaire (BAFT)Herzberg, K. N., Sheppard, S. C., Forsyth, J. P., Credé, M., Earleywine, M., & Eifert, G. H. (2012). The Believability of Anxious Feelings and Thoughts Questionnaire (BAFT): a psychometric evaluation of cognitive fusion in a nonclinical and highly anxious community sample. Psychological Assessment, 24(4), 877-891. DOI: 10.1037/a0027782
BAFT - Arabic
BAFT - ArabicBougueffa, I. (2020) فعالية العلاج بالتقبل والإلتزام في التخفيف من أعراض الوسواس القهري [The effectiveness of acceptance and commitment therapy in relieving OCD symptoms]. Dissertation, University of Batna. The Believability of Anxious Feelings and Thoughts Questionnaire (BAFT) Arabic version is in the appendix. Retrieved from http://dspace.univ-batna.dz/handle/123456789/1210
BAFT - Persian/Farsi
BAFT - Persian/FarsiMohammadipour, M., Naghinasab Ardehaee, F. A (2016). Psychometric Indices of the Farsi Version of the Believability of Anxious Feelings and Thoughts Questionnaire (BAFT). Int J Ment Health Addiction 14, 752–760. https://doi.org/10.1007/s11469-015-9624-4
Soltani E, Bahrainian , S A, Masjedi Arani A, Farhoudian A, Gachkar L. (2015) Psychometric properties of the Believability of Anxious Feelings and Thoughts Questionnaire (BAFT). pajoohande, 20 (5), 273-282.
BAFT - Spanish
BAFT - SpanishFrancisco J. Ruiz, Paula Odriozola-González, & Juan C. Suárez-Falcón (2014) The Spanish version of the Believability of Anxious Feelings and Thoughts Questionnaire. Psicothema, 26(3), 308-313. http://doi.org/10.7334/psicothema2013.221 The Spanish Translation of the BAFT is in Table 1.
Drexel Defusion Scale (DDS)
Drexel Defusion Scale (DDS)Evan M. Forman, James D. Herbert, Adrienne S. Juarascio, Peter D. Yeomans, John A. Zebell, Elizabeth M. Goetter Ethan Moitra (2012) The Drexel defusion scale: A new measure of experiential distancing. Journal of Contextual Behavioral Science, 1(1–2), 55-65. https://doi.org/10.1016/j.jcbs.2012.09.001 The Drexel Defusion Scale (DDS) is in Appendix Table A1.
DDS in Turkish
DDS in TurkishAydın, G , Güneri, O . (2021). The Drexel Defusion Scale: Reliability and Validity of the Turkish Version. Sakarya University Journal of Education, 11(1) , 67-82. http://doi.org/10.19126/suje.770582
Mindfulness Measures
Mindfulness Measures adminFive Facet Mindfulness Questionnaire (FFMQ)
Five Facet Mindfulness Questionnaire (FFMQ)The Five Facet Mindfulness Questionnaire is a 39 item measure consisting of five subscales (observing, describing, acting with awareness, non-judging of inner experience, and non-reactivity to inner experience).
FFMQ References:
- Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27-45.
- Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15, 329-342.
- Christopher, M.S., Neuser, N.J., Michael, P.G. et al. (2012). Exploring the Psychometric Properties of the Five Facet Mindfulness Questionnaire. Mindfulness, 3, 124–131. https://doi.org/10.1007/s12671-011-0086-x
- Curtiss, J. & Klemanski, D.H. (2014). Factor Analysis of the Five Facet Mindfulness Questionnaire in a Heterogeneous Clinical Sample. J Psychopathol Behav Assess, 36, 683–694. https://doi.org/10.1007/s10862-014-9429-y
- Spencer, S. D., Jo, D., Hamagami F., Antonio, M. C. K., Qinaʻau, J., Masuda, A., & Hishinuma, E. S. (2022). A psychometric validation of contextual cognitive behavioral therapy-informed measures with racially and ethnically diverse adults. Journal of Contextual Behavioral Science. https://doi.org/10.1016/j.jcbs.2022.06.004
FFMQ-Short Form References:
- Bohlmeijer, E., ten Klooster, P. M., Fledderus, M., Veehof, M., & Baer, R. (2011). Psychometric Properties of the Five Facet Mindfulness Questionnaire in Depressed Adults and Development of a Short Form. Assessment, 18(3), 308-320. https://doi.org/10.1177/1073191111408231
- Gu, J., Strauss, C., Crane, C., Barnhofer, T., Karl, A., Cavanagh, K., & Kuyken, W. (2016). Examining the factor structure of the 39-item and 15-item versions of the Five Facet Mindfulness Questionnaire before and after mindfulness-based cognitive therapy for people with recurrent depression. Psychological Assessment, 28(7), 791–802. https://doi.org/10.1037/pas0000263
- Levin-Aspenson, H.F., Marks, R.M., Dalrymple, K.L, &Zimmerman, M. (2023). Does the Five Facet Mindfulness Questionnaire measure the same constructs before and after ACT-based treatment? Examination of the longitudinal measurement invariance of the 24-item FFMQ-SF. Journal of Contextual Behavioral Science, 29, 131-139. https://doi.org/10.1016/j.jcbs.2023.07.001
FFMQ - Arabic
FFMQ - ArabicAl Awamleh, A. (2014) The effect of educational gymnastics skills on five facet mindfulness. Journal of Physical Education and Sport, 14(2), 194 - 197. http://doi.org/10.7752/jpes.2014.02030
Mazahreh, J. & Al Awamleh, A. (2016) The relationship between mindfulness, self compassion and the level of skill performance of gymnastics players. Sport Science, 9(2), 29‐33.
Mousa Ahamad, M., Saada, B., Alshamaileh, Q., Abusamra, M. & Al-Awamleh, A. (2018) The Level of Mindfulness, Hand-eye Coordination and Strength among Elite Fencers. Asian Social Science, 14(4), 65-69. https://doi.org/10.5539/ass.v14n4p65
Ebtsam Ahmed Mohamed, Safaa Mohammed Zaki, & Fatma Nagy Kotb (2021) Assessment of Mindfulness among Head Nurses, and its Effect on Staff Nurses’ Emotional Regulation and Quality of Work Life. Assiut Scientific Nursing Journal, 9(24), 153- 165. https://doi.org/10.21608/asnj.2021.58417.1103
FFMQ - Bosnian
FFMQ - BosnianAlispahic, S., & Hasanbegovic-Anic, E. (2017). Mindfulness: Age and gender differences on a Bosnian sample. Psychological Thought, 10(1), 155–166. https://doi.org/10.5964/psyct.v10i1.224 Retrieved from www.psycharchives.org/bitstream/20.500.12034/1497/1/psyct.v10i1.224.pdf
The FFMQ Bosnian version is in the appendix.
Hasanbegović-Anić, Enedina & Alispahic, Sabina & Tuce, Đenita & Čolić, Jasmin. (2017). Petofaktorski upitnik svjesne usredotočenosti: Provjera nekih metrijskih karakteristika na općoj populaciji/Five factor mindfulness questionnaire: examination of some metric characteristic in general population.
FFMQ - Chinese
FFMQ - ChineseDeng, YQ., Liu, XH., Rodriguez, M.A. et al. (2011) The Five Facet Mindfulness Questionnaire: Psychometric Properties of the Chinese Version. Mindfulness, 2, 123–128. https://doi.org/10.1007/s12671-011-0050-9
Hou, J., Wong, S. Y.-S., Lo, H. H.-M., Mak, W. W.-S., & Ma, H. S.-W. (2014). Validation of a Chinese Version of the Five Facet Mindfulness Questionnaire in Hong Kong and Development of a Short Form. Assessment, 21(3), 363–371. https://doi.org/10.1177/1073191113485121
Huang, F.-Y., Wu, C.-W., Bhikshu, H.-M., Shih, G.-H., Chao, Y.-P., and Dai, C.-T. (2015). Validation of the Taiwanese Version of the Five Facet Mindfulness Questionnaire (T-FFMQ). Psychological Testing, 62, 231–260. Retrieved from https://pt.ntcu.edu.tw/PQS/Home/doc?id=63
Meng, Y., Mao, K. & Li, C. (2020). Validation of a Short-Form Five Facet Mindfulness Questionnaire Instrument in China. Front. Psychol., 10, 3031. DOI: 10.3389/fpsyg.2019.03031
FFMQ - Croatian
FFMQ - CroatianGračanin, A., Gunjača, V., Tkalčić, M., Kardum, I., Bajšanski, I. and Perak, B. (2017). The structure of focused awareness and its connection to personality traits and emotional response. Psychological Topics, 26 (3), 675-700. https://doi.org/10.31820/pt.26.3.9
FFMQ - Czech
FFMQ - CzechKorinek, D. & Benda, J. & Žitník, J. (2019). Psychometrické charakteristiky krátké české verze Dotazníku pěti aspektů všímavosti (FFMQ-15-CZ). [Psychometric characteristics of the short Czech version of the five facet mindfulness questionnaire] Ceskoslovenska Psychologie, 63(1), 55-70.
Retrieved from https://www.researchgate.net/publication/331210436_Psychometricke_charakteristiky_kratke_ceske_verze_Dotazniku_peti_aspektu_vsimavosti_FFMQ-15-CZ
The Czech translation of the FFMQ-15 items is in the article.
FFMQ - Danish
FFMQ - DanishJensen, C. G., Krogh, S. C., Westphael, G., & Hjordt, L. V. (2019). Mindfulness is positively related to socioeconomic job status and income and independently predicts mental distress in a long-term perspective: Danish validation studies of the Five-Factor Mindfulness Questionnaire. Psychological Assessment, 31(1), e1–e20. https://doi.org/10.1037/pas0000667
FFMQ - Dutch
FFMQ - DutchVeehof, M.M., ten Klooster, P.M., Taal, E. et al. (2011). Psychometric properties of the Dutch Five Facet Mindfulness Questionnaire (FFMQ) in patients with fibromyalgia. Clin Rheumatol, 30, 1045–1054. https://doi.org/10.1007/s10067-011-1690-9
Verhenne, Fanya (2010) Validiteit van de Five Facet Mindfulness questionnaire (FFMQ) bij mensen met fibromyalgie. Retrieved from http://essay.utwente.nl/60543/
The FFMQ Dutch Translation is in the appendix.
FFMQ - Estonian
FFMQ - EstonianTeri Talpsep (2015) MEASURING MINDFULNESS AND SELF-COMPASSION: A QUESTIONNAIRE AND ERP STUDY. Master’s Thesis, University of Tartu. DOI: 10.1.1.824.992
The Estonian version of the FFMQ is in the Appendix.
FFMQ - French
FFMQ - FrenchHeeren, A., Douilliez, C., Peschard, V., Debrauwere, L., & Philippot, P. (2011). Cross-cultural consistency of the Five Facets Mindfulness Questionnaire: Adaptation and validation in a French sample. European Review of Applied Psychology, 61, 147-151
Abstract:
Introduction. – Recent research has revealed that mindfulness training improves mental health and psychological functioning. Although several questionnaires have been developed to measure mindfulness, the Five Facets Mindfulness Questionnaire (FFMQ), [Baer et al., 2006. Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45] is currently one of the most empiricallybased scale assessing mindfulness.
Objective. – The present study was designed to: (1) test the psychometric properties and (2) explore the structural validation of the French version of the FFMQ.
Method. – Two hundred and fourteen participants were tested using the French version of the FFMQ.
Results. – Using confirmatory factor analysis, the results showed the French version of the FFMQ has good psychometric properties and a structural validity similar to the initial version.
Conclusion. – This adaptation constituted a validated mindfulness measure for French-speaking clinicians as well as researchers.
Keywords: Mindfulness, FFMQ, validation, French-speaking sample, self-report assessment, confirmatory factor analysis
Résumé
Introduction. Des recherches récentes indiquent que l’apprentissage de la pleine conscience améliore la santé mentale et le fonctionnement psychologique. Bien qu’une série de questionnaire ont été développés en vue de mesurer ce construit, le Five Facets Mindfulness Questionnaire (FFMQ) (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) est actuellement l’un des instruments empiriquement validés le plus utilisés pour mesurer la pleine conscience.
Objectifs. La présente étude a été élaborée en vue (1) de déterminer les propriétés psychométriques et (2) d’explorer la validité structurelle d’une adaptation francophone du FFMQ.
Méthode. Deux-cents quatorze participants ont complétés l’adaptation francophone du FFMQ.
Résultats. Au moyen d’analyses factorielles confirmatoires, les résultats indiquent que la version francophone du FFMQ présente de bonnes propriétés psychométriques et une validité structurale similaire à la version initiale.
Conclusion. La présente adaptation constitue une mesure valide d’évaluation de la pleine conscience utilisable tant pour le clinicien que le chercheur francophone.
Mots-clés: Pleine conscience, FFMQ, validation, échantillon francophone, questionnaire, analyse factorielle confirmatoire
FFMQ - French version
FFMQ - French version Alexandre HeerenFFMQ - German
FFMQ - GermanMichalak, J. et al. (2016). Erfassung von Achtsamkeit mit der deutschen Version des Five Facet Mindfulness Questionnaires (FFMQ-D). Zeitschrift für Gesundheitspsychologie, 24(1), 1-12. https://doi.org/10.1026/0943-8149/a000149 FFMQ German Translation is in Tabelle 2.
FFMQ - Hebrew
FFMQ - HebrewHAGIT AARONSOHN (2012) META-MIND VS. META- EMOTION: THE IMPACT OF MINDFULNESS MEDITATION PRACTICE ON EMOTIONAL PROCESSING AND EMOTIONAL SCHEMAS. THESIS: BEN-GURION UNIVERSITY OF THE NEGEV.
Retrieved from http://aranne5.bgu.ac.il/others/AaronsohnHagit.pdf
The FFMQ Hebrew Translation is in the Appendix Page XLIX.
FFMQ - Hungarian
FFMQ - HungarianJózsa L. Az Ötfaktoros Jelentudatosság Kérdőív (FFMQ) adaptálása magyar mintán. In: Rózsa S, Kálmán R, Kő N, Nagy H, Fiáth T, Magi A, Eisinger A, Oláh A. Az érzelmi arcfelismerés jelentősége és mérése a pszichológiai kutatásokban: Az Ekman-féle érzelmi detekció teszttel szerzett hazai tapasztalatok. Pszichológia, 2012; 32, 229-251. https://doi.org/10.1556/pszicho.32.2012.3.4
FFMQ - Icelandic
FFMQ - IcelandicFrostadottir, A.D. & Dorjee, D. (2019). Effects of Mindfulness Based Cognitive Therapy (MBCT) and Compassion Focused Therapy (CFT) on Symptom Change, Mindfulness, Self-Compassion, and Rumination in Clients With Depression, Anxiety, and Stress. Frontiers in Psychology. https://www.frontiersin.org/article/10.3389/fpsyg.2019.01099
FFMQ - Italian
FFMQ - ItalianGiovannini, C., Giromini, L., Bonalume, L. et al. (2014). The Italian Five Facet Mindfulness Questionnaire: A Contribution to its Validity and Reliability. Journal of Psychopathology and Behavioral Assessment, 36, 415–423. https://doi.org/10.1007/s10862-013-9403-0
FFMQ - Japanese
FFMQ - JapaneseFive Facet Mindfulness Questionnaire (FFMQ) is a measure of mindfulness that holds an important position in ACT. Many measurement scales for mindfulness have been published in recent years, but FFMQ is the result of joint factor analysis.
The Japanese version of FFMQ has a five-factor structure (observing, describing, acting with awareness, nonjudging, nonreactivity).
Sugiura, Y., Sato, A., Ito, Y., Murakami, H. (2012). Development and validation of the Japanese version of the Five Facet Mindfulness Questionnaire. Mindfulness, 3, 85-94.
Takahashi, T., Saito, J., Fujino, M., Sato, M., & Kumano, H. (2022). The Validity and Reliability of the Short Form of the Five Facet Mindfulness Questionnaire in Japan. Frontiers in Psychology, 13, 833381. DOI: 10.3389/fpsyg.2022.833381
The FFMQ Japanese version is on the ACBS Japan Chapter website.
FFMQ - Korean
FFMQ - KoreanChoi, S-Y.(2015). Study on Validity and Reliability of Five Facet Mindfulness Questionnaire (FFMQ) for Measuring Mindfulness Meditation Program Before and After. Journal of Oriental Neuropsychiatry, 26 (2). http://doi.org/10.7231/jon.2015.26.2.181
FFMQ - Latvian
FFMQ - LatvianMajors, Māris (2013). APZINĀTĪBAS PIECU ASPEKTU APTAUJAS (The Five Facet Mindfulness Questionarie (FFMQ)) ADAPTĀCIJA. Master's thesis. https://dspace.lu.lv/dspace/handle/7/42253
FFMQ - Norwegian
FFMQ - NorwegianDundas, I., Vøllestad, J., Binder, P. E., & Sivertsen, B. (2013). The Five Factor Mindfulness Questionnaire in Norway. Scandinavian journal of psychology, 54(3), 250–260. https://doi.org/10.1111/sjop.12044
FFMQ - Persian
FFMQ - PersianTAMANNAEIFAR, S., & ASGHARNEJADE FARID, A., & MIRZAEE, M., & SOLEIMANI, M. (2016). PSYCHOMETRIC PROPERTIES OF FIVE FACTOR MINDFULNESS QUESTIONNAIRE. DEVELOPMENTAL PSYCHOLOGY (JOURNAL OF IRANIAN PSYCHOLOGISTS), 12(47), 321-329.
FFMQ - Polish Validation
FFMQ - Polish ValidationRadoń, S. (2014). Validation of the Polish adaptation of the Five Facet Mindfulness Questionnaire. Annals of Psychology, 17 (4), 737-760.
FFMQ - Portuguese
FFMQ - PortugueseVíviam Vargas de Barros, Elisa Harumi Kozasa, Isabel Cristina Weiss de Souza, Telmo Mota Ronzani (2014) Validity evidence of the brazilian version of the five facet mindfulness questionnaire (FFMQ). Psicologia: Teoria e Pesquisa, 30 (3). https://doi.org/10.1590/S0102-37722014000300009
Alexandre Ramos, António Rosado, Sidónio Serpa, Adolfo Cangas, José Gallego, Luís Ramos (2018). Validity evidence of the portuguese version of the five facet mindfulness questionnaire. Revista de Psicología del Deporte, 27(2), 87–98. Available at: https://archives.rpd-online.com/article/view/v27-n2-carvalho-ramos-rosado-etal.html
FFMQ - Romanian
FFMQ - RomanianElena Druică & Rodica Ianole (2018). Simply Clustering. Making New Sense In The Five Facets Mindfulness Questionnaire. Romanian Statistical Review, nr. 1.
FFMQ - Russian
FFMQ - RussianGolubev, A. M. & Dorosheva, E. A. (2018) Особенности применения русскоязычной версии пятифакторного опросника осознанности. [Features of the Russian-language version of the five-factor questionnaire of awareness}. Сибирский психологический журнал, 69,46–68.
FFMQ - Sinhala
FFMQ - SinhalaBaminiwatta, A., Alahakoon, H., Herath, N.C. et al. (2022). Psychometric Evaluation of a Sinhalese Version of the Five Facet Mindfulness Questionnaire and Development of a Six-Facet Short Form in a Sri Lankan Buddhist Context. Mindfulness 13, 1069–1082. https://doi.org/10.1007/s12671-022-01863-1
Outschoorn, N.O., Herath, H. & Amarasuriya, S.D. (2021) SINHALA VERSION OF THE FIVE FACET MINDFULNESS QUESTIONNAIRE (FFMQ-39-SIN): CONTENT VALIDATION THROUGH EXPERT JUDGEMENT AND INTERNAL CONSISTENCY. Proceeding of the Open University Research Sessions. Retrieved from https://ours.ou.ac.lk/wp-content/uploads/2021/11/ID-134_SINHALA-VERSION-OF-THE-FIVE-FACET-MINDFULNESS-QUESTIONNAIRE-FFMQ-39-SIN-CONTENT-VALIDATION-THROUGH-EXPERT-JUDGEMENT-AND-INTERNAL-CONSISTENCY.pdf
FFMQ - Slovak
FFMQ - SlovakLátalová, Veronika & Pilárik, Ľubor. (2014). Overenie psychometrických vlastností a faktorovej štruktúry slovenskej verzie dotazníka FFMQ (five–facet mindfulness questionnaire) [The evaluation of the psychometric properties and the factor structure of the slovak version of the questionnaire FFMQ (five-facet mindfulness questionnaire)]. Psychologie a její kontexty, 5(2), 81–99. Retrieved from https://www.researchgate.net/publication/267506585
FFMQ - Spanish
FFMQ - SpanishAsensio-Martínez Á, Masluk B, Montero-Marin J, Olivan-Blázquez B, Navarro-Gil MT, García-Campayo J, et al. (2019) Validation of Five Facets Mindfulness Questionnaire – Short form, in Spanish, general health care services patients sample: Prediction of depression through mindfulness scale. PLoS ONE,14(4), e0214503. https://doi.org/10.1371/journal.pone.0214503
Aguado, J., Luciano, J.V., Cebolla, A., Serrano-Blanco, A., Soler, J. & García-Campayo, J. (2015). Bifactor analysis and construct validity of the five facet mindfulness questionnaire (FFMQ) in non-clinical Spanish samples. Front. Psychol., 6, 404. DOI: 10.3389/fpsyg.2015.00404
Cebolla, A., García-Palacios, A., Soler, J., Guillen, V., Baños, R. Botella, C. (2012). Psychometric properties of the Spanish validation of the Five Facets of Mindfulness Questionnaire (FFMQ). Eur. J. Psychiat., 26(2), 118-126. https://dx.doi.org/10.4321/S0213-61632012000200005
FFMQ - Swedish
FFMQ - SwedishJosefine L. Lilja, Annika Frodi-Lundgren, Jan Johansson Hanse, Torbjörn Josefsson, Lars-Gunnar Lundh, Camilla Sköld, Erling Hansen & Anders G. Broberg (2011) Five Facets Mindfulness Questionnaire—Reliability and Factor Structure: A Swedish Version. Cognitive Behaviour Therapy, 40(4), 291-303. DOI: 10.1080/16506073.2011.580367
FFMQ - Turkish
FFMQ - TurkishHandan Deniz Ayalp & Nesrin Hisli Şahin (2018) Beş Faktörlü Bilgece Farkındalık Ölçeği-Kısa Formu’nun (BFBFÖ-K) Türkçe Uyarlaması [Turkish adaptation of the Five Facet Mindfulness Questionnaire - Short Form (FFMQ-S)]. Klinik Psikoloji Dergisi, 2018, Issue 3, 117-127.
Fatoş Kınay (2013) BEŞ BOYUTLU BİLİNÇLİ FARKINDALIK ÖLÇEĞİ’Nİ TÜRKÇE’YE UYARLAMA, GEÇERLİK VE GÜVENİRLİK ÇALIŞMASI. İSTANBUL BİLİM ÜNİVERSİTESİ SOSYAL BİLİMLER ENSTİTÜSÜ, Master's Thesis.
FFMQ - Ukrainian
FFMQ - UkrainianKaplunenko, Y. & Kuchyna, V. (2022). АДАПТАЦІЯ ТА ВАЛІДИЗАЦІЯ ПʼЯТИФАКТОРНОГО ОПИТУВАЛЬНИКА МАЙНДФУЛНЕС (ПОМ-39) [ADAPTATION AND VALIDATION OF FIVE FACTOR MINDFULNESS QUESTIONNAIRE]. International Journal of Innovative Technologies in Social Science, 1(33). https://doi.org/10.31435/rsglobal_ijitss/30032022/7795 The FFMQ Ukrainian version is in the appendix.
FFMQ - Urdu
FFMQ - UrduSayyeda Taskeen Zahra & Saima Riaz (2017) MEDIATING ROLE OF MINDFULNESS IN STRESSRESILIENCE RELATIONSHIP AMONG UNIVERSITY STUDENTS. Pakistan Journal of Psychology, 48(2), 21-32.
FFMQ - Vietnamese
FFMQ - VietnameseNguyen, H.T.M., Nguyen, H.V. & Bui, T.T.H. (2022). The psychometric properties of the Vietnamese Version of the Five Facet Mindfulness Questionnaire. BMC Psychology, 10, 300. https://doi.org/10.1186/s40359-022-01003-3
Freiburg Mindfulness Inventory (FMI)
Freiburg Mindfulness Inventory (FMI)The FMI scale and measure development article are attached below.
FMI - Arabic
FMI - ArabicZeinab Bitar, Feten Fekih Romdhane, Radoslaw Rogoza, Hossam M. Ghorab, Sahar Obeid & Souheil Hallit (2023 in press) Psychometric properties of the short form of the Freiburg Mindfulness Inventory in the Arabic language, International Journal of Environmental Health Research. DOI: 10.1080/09603123.2023.2267483
Bougueffa, I. (2020) فعالية العلاج بالتقبل والإلتزام في التخفيف من أعراض الوسواس القهري [The effectiveness of acceptance and commitment therapy in relieving OCD symptoms]. Dissertation, University of Batna. The Freiburg Mindfulness Inventory (FMI) Arabic version is in the appendix. Retrieved from http://dspace.univ-batna.dz/handle/123456789/1210
FMI - Brazilian Portguese
FMI - Brazilian PortgueseHirayama, M.S. (2014) Freiburg Mindfulness Inventory: adaptação cultural e validação para a língua portuguesa no Brasil. [Freiburg Mindfulness Inventory : cross-cultural adaptation and validation to Portuguese in Brasil] Tese (doutorado) - Universidade Estadual de Campinas, Faculdade de Enfermagem, Campinas, SP. Disponível em: http://www.repositorio.unicamp.br/handle/REPOSIP/283892
Hirayama, M.S. et al (2014) A percepção de comportamentos relacionados à atenção plena e a versão brasileira do Freiburg Mindfulness Inventory. [The perception of behavior related to mindfulness and the Brazilian version of the Freiburg Mindfulness Inventory]. Ciênc. saúde coletiva 19 (9). https://doi.org/10.1590/1413-81232014199.12272013 The Freiburg Mindfulness Inventory adapted for Brazil (FMI-Br) is in Quadro 2.
FMI - Chinese
FMI - ChineseChen, S.Y., & Zhou, R.L. (2014). Validation of a Chinese Version of the Freiburg Mindfulness Inventory–Short Version. Mindfulness, 5, 529–535. https://doi.org/10.1007/s12671-013-0208-8
FMI - Danish
FMI - DanishJensen, C. G., Niclasen, J., Vangkilde, S. A., Petersen, A., & Hasselbalch, S. G. (2016). General inattentiveness is a long-term reliable trait independently predictive of psychological health: Danish validation studies of the Mindful Attention Awareness Scale. Psychological Assessment, 28(5), e70–e87. https://doi.org/10.1037/pas0000196
FMI - Dutch
FMI - DutchBruggeman-Everts, F. Z., Van der Lee, M. L., Van ‘t Hooft, E. F. M., & Nyklíček, I. (2017). Validation of the Dutch Freiburg Mindfulness Inventory in Patients With Medical Illness. SAGE Open. https://doi.org/10.1177/2158244017705936 The FMI Dutch translation is in the Supplemental Material.
FMI - French
FMI - FrenchTrousselard, M., Steiler, D., Raphel, C. et al. (2010) Validation of a French version of the Freiburg Mindfulness Inventory - short version: relationships between mindfulness and stress in an adult population. BioPsychoSocial Med, 4, 8. https://doi.org/10.1186/1751-0759-4-8 The FMI French Translation is in the Electronic supplementary material.
FMI - German
FMI - GermanHeidenreich, T., Ströhle, G., & Michalak, J. (2006). Achtsamkeit: Konzeptuelle aspekte und ergebnisse zum Freiburger achtsam-keitsfragebogen [Conceptual aspects and results of the Freiburg mindfulness questionnaire]. Verhaltenstherapie, 16(1), 33-40. http://doi.org/10.1159/000091521
FMI - Italian
FMI - ItalianFreiburg Mindfulness Inventory (FMI)
Walach, H., Buchheld, N., Buttenmüller, V., Kleinknecht, N., & Schmidt, S. (2006). Measuring mindfulness - the Freiburg Mindfulness Inventory (FMI). Personality and Individual Differences, 40(8), 1543-1555.
Traduzione Italiana (1.0) a cura di Cioci, M., Rossi, E., Violini, P., Francesconi, C., Ristè, N., Melchiorri, E. (2013) AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (2.0) a cura di Rossi, E., Melchiorri, E., Lijoi, E., Ristè, N., Violini, P., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Violini, P., Ristè, N., Lijoi, E., Melchiorri, E., Rossi, E., Panzera, A.,(2014). The preliminary psychometric properties of an Italian version of Freiburg Mindfulness Inventory (FMI) for Adolescents. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014
Per informazioni: segreteria@aiscc.it – www.aiscc.it
FMI - Persian
FMI - PersianGhasemi Jobaneh R, Arab Zadeh M, Jalili Nikoo S, Mohammad Alipoor Z, & Mohsenzadeh F. (2015). بررسی روایی و پایایی نسخه فارسی فرم کوتاه پرسشنامه ذهنآگاهی فرایبورگ. [Survey the validity and reliability of the persian version of short form of freiburg mindfulness inventory.] Journal of Rafsanjan University of Medical Science, 14(2), 137- 50. http://eprints.rums.ac.ir/5689/
FMI - Polish
FMI - PolishBaran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
See attachment for Polish FMI.
FMI - Spanish
FMI - SpanishPérez-Verduzco, G., & Laca-Arocena, F. A. (2017). Traducción y validación de la versión abreviada del Freiburg Mindfulness Inventory (FMI-14). Revista Evaluar, 17(1). https://doi.org/10.35670/1667-4545.v17.n1.17076
Arocena, Francisco & Pérez-Verduzco, Germán & Valencia, Angel. (2016). Multivariate Analysis of the Spanish Version of the FMI-14: Contributions From the Item Response Theory and Biplot Methods. PAPIREX Indian Journal of Research, 5, 242-245.
FMI - Turkish
FMI - TurkishHasan Turan Karatepe & Kaasım Fatih Yavuz (2019) Reliability, validity, and factorial structure of the Turkish version of the Freiburg Mindfulness Inventory (Turkish FMI). Psychiatry and Clinical Psychopharmacology, 29(4), 472-478. http://doi.org/10.1080/24750573.2019.1663582
FMI - Ukrainian
FMI - UkrainianСахнюк Роксолана Володимирівна (2021). Психометричні властивості української версії Фрайбурзького опитувальника майндфулнес на вибірці повнолітнього. Магістерська робота, Український католицький університет. [Sakhniuk R.V. (2021). Psychometric properties of the Ukrainian version of Freiburg Mindfulness questionnaire on a sample of adults. Master's thesis, Ukrainian Catholic University.] The FMI Ukrainian version is in the appendix. http://www.er.ucu.edu.ua/bitstream/handle/1/2763/Sakhniuk_mag.pdf
Kentucky Inventory of Mindfulness Skills (KIMS)
Kentucky Inventory of Mindfulness Skills (KIMS)Baer, R.A., Smith, G.T., & Allen, K.B. (2004) Assessment of Mindfulness by Self-Report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11(3), 191-206. http://doi.org/10.1177/1073191104268029
The KIMS is available on ruthbaer.com.
KIMS - Arabic
KIMS - ArabicAldahadha, B. (2013). The effects of Muslim praying meditation and transcendental meditation programs on mindfulness among the University of Nizwa students. College Student Journal, 47, 668-676.
KIMS - Chinese
KIMS - ChineseXin Xu, Daxing Wu, Xiaohua Zhao, Junxiang Chen, Jie Xia, Mulei Li, Xueqing Nie & Xue Zhong (2016) Relation of perceptions of educational environment with mindfulness among Chinese medical students: a longitudinal study. Medical Education Online, 21(1). DOI: 10.3402/meo.v21.30664
KIMS - Dutch
KIMS - DutchDekeyser, M., Raes, F., Leijssen, M., Leysen, S., & Dewulf, D. (2008) Mindfulness skills and interpersonal behaviour. Personality and Individual Differences, 44(5), 1235-1245. https://doi.org/10.1016/j.paid.2007.11.018
KIMS - French
KIMS - FrenchNicastro, R., Jermann, F., Bondolfi, G., & McQuillan, A. (2010). Assessment of Mindfulness With the French Version of the Kentucky Inventory of Mindfulness Skills in Community and Borderline Personality Disorder Samples. Assessment, 17(2), 197–205. https://doi.org/10.1177/1073191110363551
KIMS - German
KIMS - GermanStröhle, G., Nachtigall, C., Michalak, J., Heidenreich, T. (2010). Die Erfassung von Achtsamkeit als mehrdimensionales Konstrukt: Die deutsche Version des Kentucky Inventory of Mindfulness Skills (KIMS-D) [Measuring mindfulness as a multidimensional construct: German version of the Kentucky Inventory of Mindfulness Skills (KIMS-D)]. Zeitschrift Für Klinische Psychologie Und Psychotherapie, 39(1), 1-12. https://doi.org/10.1026/1616-3443/a000001
KIMS - Greek
KIMS - GreekPsarraki, E.E. et al. (2021). The Kentucky Inventory of Mindfulness Skills in Greek Undergraduate and Postgraduate Students. In: Vlamos, P. (eds) GeNeDis 2020. Advances in Experimental Medicine and Biology, vol 1339. Springer, Cham. https://doi.org/10.1007/978-3-030-78787-5_28
KIMS - Korean
KIMS - KoreanKim Jong-mo. (2006). 한국판 켄터키 마음챙김기술 척도의 타당화 연구 [A Validation Study of Korean Version of Kentucky Inventory of Mindfulness Skills]. Korean Journal of Clinical Psychology, 25, 4, 1123-1139.
KIMS - Persian
KIMS - PersianDEHGHAN MANSHADI ZOBEYDEH et al (2012) PSYCHOMETRIC CHARACTERISTICS OF THE KENTUCKY INVENTORY OF MINDFULNESS SKILLS. JOURNAL OF THOUGHT & BEHAVIOR IN CLINICAL PSYCHOLOGY, 7(25), 27 - 36. https://www.sid.ir/en/journal/ViewPaper.aspx?ID=372692
KIMS - Slovenian
KIMS - SlovenianČernetič Mihael (2016) The relationship between anxiety and mindfulness: The role of mindfulness facets, implicit anxiety, and the problem of measuring anxiety by self-report. Psihologija, 49(2), 169-183. https://doi.org/10.2298/PSI1602169C
KIMS - Spanish
KIMS - SpanishRuiz, F. J. (2014). The relationship between low levels of mindfulness skills and pathological worry: The mediating role of psychological inflexibility. [La relación entre habilidades de mindfulness y preocupación patológica: El rol mediador de la inflexibilidad psicológica]. Anales de Psicología / Annals of Psychology, 30(3), 887–897. https://doi.org/10.6018/analesps.30.3.150651
KIMS - Swedish
KIMS - SwedishErling Hansen, Lars‐Gunnar Lundh, Anders Homman & Margit Wångby‐Lundh (2009). Measuring Mindfulness: Pilot Studies with the Swedish Versions of the Mindful Attention Awareness Scale and the Kentucky Inventory of Mindfulness Skills. Cognitive Behaviour Therapy, 38(1), 2-15. http://doi.org/10.1080/16506070802383230
KIMS-R - Basque
KIMS-R - BasqueOlarza, A., Soroa, G., Aritzeta, A. et al. (2023 in press). Basque Adaptation of the Reduced Kentucky Inventory of Mindfulness Skills (KIMS-R). Mindfulness. https://doi.org/10.1007/s12671-023-02241-1
Mindful Attention Awareness Scale (MAAS)
Mindful Attention Awareness Scale (MAAS)The Mindful Attention Awareness Scale (MAAS) is a 15 item measure assessing mindfulness of moment to moment experience.
Reference: Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822-848.
MAAS - Arabic
MAAS - ArabicMarei S. Younes & Mohammed R. Alzahrani (2018) Could Resilience and Flourishing be Mediators in the Relationship between Mindfulness and Life Satisfaction for Saudi College Students? A Psychometric and Exploratory Study. Journal of Educational and Psychological Studies, 12(4), 708-723. https://doi.org/10.24200/jeps.vol12iss4pp708-723
MAAS - Chinese
MAAS - ChineseBlack, D. S., Sussman, S., Johnson, C. A., & Milam, J. (2012). Psychometric Assessment of the Mindful Attention Awareness Scale (MAAS) Among Chinese Adolescents. Assessment, 19(1), 42–52. https://doi.org/10.1177/1073191111415365
Deng, YQ., Li, S., Tang, YY. et al. (2012) Psychometric Properties of the Chinese Translation of the Mindful Attention Awareness Scale (MAAS). Mindfulness 3, 10–14. https://doi.org/10.1007/s12671-011-0074-1
Chen, S., Cui, H., Zhou, R., and Jia, Y. (2012). Revision and reliability and validity of the Mindfulness Attention Awareness Scale (MASS). Chin. J. Clin. Psych. 20, 148–151. DOI: 10.16128/j.cnki.1005-3611.2012.02.024
MAAS - Danish
MAAS - DanishJensen, C. G., Niclasen, J., Vangkilde, S. A., Petersen, A., & Hasselbalch, S. G. (2016). General inattentiveness is a long-term reliable trait independently predictive of psychological health: Danish validation studies of the Mindful Attention Awareness Scale. Psychological Assessment, 28(5), e70–e87. https://doi.org/10.1037/pas0000196
MAAS - Dutch
MAAS - Dutchde Bruin, E.I., Zijlstra, B.J.H., van de Weijer-Bergsma, E. et al. (2011) The Mindful Attention Awareness Scale for Adolescents (MAAS-A): Psychometric Properties in a Dutch Sample. Mindfulness, 2, 201–211. https://doi.org/10.1007/s12671-011-0061-6
MAAS - Estonian
MAAS - EstonianSeema, R., Quaglia, J.T., Brown, K.W. et al. (2015) The Estonian Mindful Attention Awareness Scale: Assessing Mindfulness Without a Distinct Linguistic Present Tense. Mindfulness, 6, 759–766. https://doi.org/10.1007/s12671-014-0314-2
MAAS - Finnish
MAAS - FinnishSuvi Naukkarinen, Petri Karkkola, Matti Kuittinen & Hannu Räty (2016). Suomenkielisen MAAS-mittarin psykometrinen rakenne ja yhteydet persoonallisuuspiirteisiin sekä hyvinvointiin. PSYKOLOGIA, 51 (05).
MAAS - French
MAAS - FrenchJermann, F., Billieux, J., Larøi, F., d'Argembeau, A., Bondolfi, G., Zermatten, A., & Van der Linden, M. (2009). Mindful Attention Awareness Scale (MAAS): Psychometric properties of the French translation and exploration of its relations with emotion regulation strategies. Psychological Assessment, 21(4), 506–514. https://doi.org/10.1037/a0017032
Adaptation de "Mindfulness Attention Awareness Scale" de Brown & Ryan (2003) inclus dans le livre de "ACT for anxiety disorders" de Eifert & Forsyth (2005). Le questionnaire est accessible en devenant membre d'ACT. Cette version française du questionnaire n'a pas été validée et il est le résultat d'une adaptation personnelle. Il n'a donc pas passé par toutes les étapes de traductions habituelles. Je l'utilise comme moyen d'orienter plus précisément la thérapie ou comme outil thérapeutique. Il ne peut donc pas être utilisé dans le cadre de recherche scientifique. Login to your ACBS account to see the attachment.
MAAS - German
MAAS - GermanMichalak, J. & Heidenreich, T. & Ströhle, G. (2008). Die deutsche Version der Mindful Attention and Awareness Scale (MAAS) Psychometrische Befunde zu einem Achtsamkeitsfragebogen. Zeitschrift Fur Klinische Psychologie Und Psychotherapie - Z KLIN PSYCHOL PSYCHOTHERY, 37, 200-208. http://doi.org/10.1026/1616-3443.37.3.200
MAAS - Greek
MAAS - GreekMantzios, M., Wilson, J.C. & Giannou, K. (2015) Psychometric Properties of the Greek Versions of the Self-Compassion and Mindful Attention and Awareness Scales. Mindfulness, 6, 123–132. https://doi.org/10.1007/s12671-013-0237-3
MAAS - Hungarian
MAAS - HungarianSimor, P., Petke, Z., & Köteles, F. (2013) Measuring pre-reflexive consciousness: The Hungarian validation of the Mindful Attention Awareness Scale (MAAS). Learning & Perception, Volume 5, Issue Supplement-2. https://doi.org/10.1556/lp.5.2013.suppl2.2
MAAS - Italian
MAAS - ItalianMindful Attention Awareness Scale (MAAS)
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822-848.
Traduzione Italiana (2.0) a cura di Lijoi, E., Ristè, N., Melchiorri, E., Rossi, E., Violini, P., Violini, P., (2014) AISCC, Gruppo Ricerca ACT.
Rabitti, E., Miselli, G., and Moderato, P. (2013). Misurare la capacità di restare in contatto con il momento presente: la validazione italiana della mindful attention awareness scale. Psicoterapia Cognitiva e Comportamentale, 19, 323-339.
Referenza bibliografica: Violini, P., Lijoi, E., Ristè, N., Rossi, E., Melchiorri, E., Panzera, A., (2014). Reliability and Validity of an Italian version of the Mindful Attention Awareness Scale (MAAS) for Youth. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
MAAS - Japanese
MAAS - JapaneseMasahiro Fujino, Shogo Kajimura, Michio Nomura (2015) Development and Validation of the Japanese Version of the Mindful Attention Awareness Scale Using Item Response Theory Analysis. The Japanese Journal of Personality, 24(1), 61-76. https://doi.org/10.2132/personality.24.61
MAAS - Korean
MAAS - KoreanKwon Sun-joung, Kim Kyung-heon. (2007) 한국판 마음챙김 주의 알아차림 척도 (K-MAAS)의 타당화 연구 [Validation of the Korean Version of Mindful Attention Awareness Scale (K-MAAS)]. Journal of Korean Psychology: Health, 12, 1, 269-287.
MAAS - Malay
MAAS - MalayPhang, C.-K., Mukhtar, F., Ibrahim, N. & Mohd. Sidik, S. (2016). Mindful Attention Awareness Scale (MAAS): factorial validity and psychometric properties in a sample of medical students in Malaysia. The Journal of Mental Health Training, Education and Practice, 11(5), 305-316. https://doi.org/10.1108/JMHTEP-02-2015-0011
Zainal, N.Z., Nor-Aziyan, Y., & Subramaniam P. (2015) Psychometric properties of the Malay-translated Mindfulness, Attention and Awareness Scale (MAAS) in a group of nursing students in Malaysia. Malaysian J Psychiatry, 24(1). https://www.mjpsychiatry.org/index.php/mjp/article/view/352
MAAS - Polish
MAAS - PolishRadoń, S. (2014). Walidacja Skali Świadomej Obecności [VALIDATION OF THE POLISH VERSION OF MINDFUL ATTENTION AWARENESS SCALE]. Studia Psychologica: Theoria et praxis, 14(1), 50-69.
MAAS - Portguese
MAAS - PortgueseGregório, S., & Pinto-Gouveia, J. (2013). Mindful attention and awareness: Relationships with psychopathology and emotion regulation. The Spanish Journal of Psychology, 16, 1-10. http://doi.org/10.1017/sjp.2013.79
MAAS - Serbian
MAAS - SerbianThe Mindful Attention Awareness Scale (MAAS) Serbian Translation can be found on the Repository of psychological instruments in Serbian [Repozitorijum psiholoških instrumenata na srpskom jeziku] (REPOPSI). http://mfr.de-1.osf.io/render?url=https://osf.io/46gq5/?direct%26mode=render%26action=download%26mode=render
https://doi.org/10.17605/OSF.IO/5ZB8P
MAAS - Slovenian
MAAS - SlovenianČernetič Mihael (2016). The relationship between anxiety and mindfulness: The role of mindfulness facets, implicit anxiety, and the problem of measuring anxiety by self-report. Psihologija, 49(2), 169-183. https://doi.org/10.2298/PSI1602169C
MAAS - Spanish
MAAS - SpanishSoler, J., Tejedor, R., Feliu-Soler, A., Pascual, J.C, Cebolla, A., Álvarez, E., & Pérez, V. (2012). Propiedades psicométricas de la versión española de la escala Mindful Attention Awareness Scale (MAAS) [Psychometric properties of the Spanish versión of the Mindful Attention Awareness Scale (MAAS)]. Actas Españolas de Psiquiatría, 40, 18-25.
Barajas, S. & Garra, L. (2014). Mindfulness and psychopathology: Adaptation of the Mindful Attention Awareness Scale (MAAS) in a Spanish sample. Mindfulness y psicopatología: adaptación de la escala de conciencia y atención plena (MAAS) en una muestra española. Clínica y Salud, 1, 49-56. https://doi.org/10.1016/S1130-5274(14)70026-X The Spanish MAAS translation is in the Appendix.
MAAS - Swedish
MAAS - SwedishErling Hansen, Lars‐Gunnar Lundh, Anders Homman & Margit Wångby‐Lundh (2009). Measuring Mindfulness: Pilot Studies with the Swedish Versions of the Mindful Attention Awareness Scale and the Kentucky Inventory of Mindfulness Skills. Cognitive Behaviour Therapy, 38(1), 2-15. http://doi.org/10.1080/16506070802383230
MAAS - Turkish
MAAS - TurkishCatak, P.D. (2012). The Turkish Version of Mindful Attention Awareness Scale: Preliminary Findings. Mindfulness, 3, 1–9. https://doi/org/10.1007/s12671-011-0072-3 The MAAS Turkish Translation is in Table 2.
MAAS - Urdu
MAAS - UrduAmna Ajmal & Syeda Shahida Batool (2020) Psychometric Properties of the Urdu Translation of Mindfulness Attention Awareness Scale (MAAS) in Pakistan. SJESR, 3(2). https://doi.org/10.36902/sjesr-vol3-iss2-2020(190-197)
Philadelphia Mindfulness Scale (PHLMS)
Philadelphia Mindfulness Scale (PHLMS)The Philadelphia Mindfulness Scale (PHLMS) is a 20 item measure consisting of 2 sub-scales (acceptance and present moment awareness).
Reference:
Cardaciotto, L., Herbert, J. D., Forman, E. M., Moitra, E., & Farrow, V. (2008). The assessment of present-moment awareness and acceptance: The Philadelphia mindfulness scale. Assessment, 15, 204-223.
PHLMS - Brazilian
PHLMS - BrazilianSilveira, A., Gomes de Castro, T. & Gomes, W. (2012). Adaptation and validation of the Philadelphia Mindfulness Scale among Brazilian adults. Psico-USF, 17, 215-223. http:doi.org/10.1590/S1413-82712012000200005
PHLMS - Chinese
PHLMS - ChineseZeng, X., Li, M., Zhang, B., & Liu, X. (2015). Revision of the Philadelphia Mindfulness Scale for measuring awareness and equanimity in Goenka's Vipassana meditation with Chinese Buddhists. Journal of religion and health, 54(2), 623–637. https://doi.org/10.1007/s10943-014-9870-y
LIANG, Y., LIU, H., ZHOU, H., WANG, D. & DENG, Y. (2018). Reliability and validity of the Chinese version of philadelphia mindfulness scale in college students. Chinese Journal of Behavioral Medicine and Brain Science, 27(9), 843-847.
PHLMS - Italian
PHLMS - ItalianPhiladelphia Mindfulness Scale (PHLMS)
Cardaciotto, L., Herbert, J. D., Forman, E. M., Moitra, E., & Farrow, V. (2008). The assessment of present-moment awareness and acceptance: The Philadelphia mindfulness scale. Assessment, 15, 204-223.
Traduzione Italiana (1.0) a cura di Ristè, N., Violini, P., Melchiorri, E., Lijoi, E., Rossi, E.,(2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Melchiorri, E.,Rossi, E., Violini, P., Ristè, N., Lijoi, E., Panzera, A., (2014). Validation of the Philadelphia Mindfulness Scale (PHLMS) for the Italian youth population. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014
Per informazioni: segreteria@aiscc.it – www.aiscc.it
PHLMS - Norwegian
PHLMS - NorwegianTom Østergaard, Tobias Lundgren, Robert D. Zettle, Nils Inge Landrø, & Vegard Øksendal Haaland (2020) Psychological Flexibility in Depression Relapse Prevention: Processes of Change and Positive Mental Health in Group-Based ACT for Residual Symptoms. Front. Psychol. https://doi.org/10.3389/fpsyg.2020.00528
PHLMS - Persian
PHLMS - PersianAmeri, S. & Kooshki, S. (2021). Psychometric Properties of the Persian Version of the Philadelphia Mindfulness Scale (PHLMS) in Students. Islamic Life Style, 5(1), 1-10. URL: http://islamiclifej.com/article-1-391-en.html
Farzin Rad, B., Rashidian, M., Shakeri Juybari, Z., & Dehghani Ashkezari, E. (2022). Investigating the Validity and Reliability of the Persian Version of the Philadelphia Mindfulness Scale (PHLMS) among Clients of Counseling and Psychotherapy Centers. Journal of Applied Psychological Research, 13(1), 345-362. DOI: 10.22059/japr.2022.319635.643768
PHLMS - Slovenian
PHLMS - SlovenianČernetič Mihael (2016). The relationship between anxiety and mindfulness: The role of mindfulness facets, implicit anxiety, and the problem of measuring anxiety by self-report. Psihologija, 49(2), 169-183. https://doi.org/10.2298/PSI1602169C
PHLMS - Spanish
PHLMS - SpanishTejedor, R. et al. (2014). Propiedades psicométricas de la versión española de la Philadelphia Mindfulness Scale [Psychometric properties of the Spanish version of the Philadelphia Mindfulness Scale] Revista de Psiquiatría y Salud Mental, 7 (4), 157-165. https://doi.org/10.1016/j.rpsmen.2014.10.002
PHLMS - Thai
PHLMS - ThaiSilpakit, Chatchawan & Silpakit, Orawan & Wisajun, Pattaraphorn. (2011). The validity of Philadelphia Mindfulness Scale Thai version. Journal of Mental Health of Thailand, 19(3), 140-147. Retrived from https://he01.tci-thaijo.org/index.php/jmht/article/view/968
The PHLMS Thai version is in the article.
PHLMS - Turkish
PHLMS - TurkishÇelik, H , Onat Kocabıyık, O . (2018). Philadelphia Farkındalık Ölçeği (PFÖ)’nin Türkçe Formunun Psikometrik Özellikleri [The Philadelphia Mindfulness Scale (PHLMS): Cultural Validity and Reliability of the Turkish Version of the PMS]. Marmara Üniversitesi Atatürk Eğitim Fakültesi Eğitim Bilimleri Dergisi, 48 (48). DOI: 10.15285/maruaebd.345925 The Turkish PMLMS items are in table 2 and table 3.
Psychological Flexibility or Inflexibility Measures
Psychological Flexibility or Inflexibility Measures CommunityAcceptance & Action Questionnaire (AAQ) and AAQ-II
Acceptance & Action Questionnaire (AAQ) and AAQ-IIThe 7-item Acceptance and Action Questionnaire - II (AAQ-II)
The AAQ-II was developed in order to establish an internally consistent measure of ACT’s model of mental health and behavioral effectiveness. Although the original AAQ (Hayes, Luoma, Bond, Masuda and Lillis, 2004), obtaining sufficient alpha levels for it has at times been a problem. It appears that there are several reasons for this (e.g., scale brevity, item wording, item selection procedures), and they were addressed in developing the AAQ-II. As a result, it is recommended that researchers and practitioners use this newer scale instead of the original AAQ (which from here forward will be termed the AAQ-I).
NOTE: The AAQ-II started out as a 10-item scale, but after final psychometric analysis has been reduced to a 7-item scale (2011). Please be sure to download the 7 item version, below.
It was designed to assess the same construct as the AAQ-I and, indeed, the two scales correlate at .97, but the AAQ-II has better psychometric consistency. The reference for the AAQ-II is:
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionniare - II: A revised measure of psychological flexibility and experiential avoidance. Behavior Therapy, 42, 676-688.
Use of the AAQ-II: Permission is given to use the AAQ-II for research and with clients, and does not require additional author permission. If, however, the AAQ-II was to be used in any type of money making enterprise (e.g., consultancy to organizations), seeking permission is requested by the authors. - Frank Bond, Goldsmiths College, London
What do we call ACT's model of mental health and behavioral effectiveness? (Or, what does the AAQ-I and -II measure?)
[Taken from Bond et al.]
When ACT was originally developed, the overarching term for its underlying model was experiential avoidance – the attempt to alter the form, frequency, or situational sensitivity of negative private events (e.g., thoughts, feelings, and physiological sensations), even when doing so leads to behavioral difficulties (Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). Acceptance was the term used to positively describe this model; thus, it is defined as the willingness to experience (i.e., not alter the form, frequency, or sensitivity of) unwanted private events, in the pursuit of one’s values and goals.
The ACT model has matured over the years, with more emphasis on the dynamic and flexible fit between context, private experiences and valued action, which have always been inherent in the model. Such flexibility is seen when ACT therapists note that sometimes persisting in behavior is helpful, while at other times changing it is helpful: it depends upon the value- and goal-related opportunities that are available in a given context. Furthermore, as other parts of the ACT model are now given emphasis (e.g., cognitive defusion, contacting the present moment, mindfulness, and perspective-taking), experiential avoidance and, hence, acceptance are taking on a narrower meaning and are being used less often as terms for the overarching model (Hayes et al., 2006). Instead, the term psychological flexibility (or flexibility) is now being used to describe this model. It is defined as the ability to fully contact the present moment and the thoughts and feelings it contains without needless defense, and, depending upon what the situation affords, persisting or changing in behavior in the pursuit of goals and values (Hayes et al., 2006). While experiential avoidance and acceptance are still useful and acceptable ways to describe this construct, psychological flexibility is the more current and overarching term. In addition, it needs to be acknowledged that in some contexts (e.g., industrial-organizational psychology) it is important to speak of this domain positively (acceptance or flexibility) and in other contexts (e.g., psychopathology) it is easier to speak of it negatively (experiential avoidance or psychological inflexibility). These differences are terminological, not substantive.
The AAQ-II and key psychometric findings for the scale can be found below. Older versions of the AAQ (i.e., AAQ-9, AAQ-16 and AAQ-49) are also listed below.
There are more specific acceptance and defusion measures available. A good measure has been developed in the area of smoking; a pain measure developed from the earliest versions of the AAQ called the Chronic Pain Acceptance Questionnaire has been published and worked very well in this area.
Several AAQ measures for specific problems and populations are posted under Disease and disorder specific AAQ variations.
There are also a variety of translated versions of the AAQ and AAQ-II posted here: AAQ-II in 30+ Languages.
Click here for a list of publications that have reviewed the AAQ and AAQ-II.
References:
- Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., Waltz, T., & Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionniare - II: A revised measure of psychological flexibility and experiential avoidance. Behavior Therapy, 42, 676-688.
- Fledderus, M., Oude Voshaar, M. A. H., ten Klooster, P. M., & Bohlmeijer, E. T. (2012). Further evaluation of the psychometric properties of the Acceptance and Action Questionnaire–II. Psychological Assessment, 24(4), 925–936. https://doi.org/10.1037/a0028200
- Flynn, M. K., Berkout, O. V., & Bordieri, M. J. (2016). Cultural considerations in the measurement of psychological flexibility: Initial validation of the Acceptance and Action Questionnaire–II among Hispanic individuals. Behavior Analysis: Research and Practice, 16(2), 81-93. https://doi.org/10.1037/bar0000035
- Renshaw, T.L. (2018). Probing the relative psychometric validity of three measures of psychological inflexibility. Journal of Contextual Behavioral Science, 7, 47-54. https://doi.org/10.1016/j.jcbs.2017.12.001
- McAndrews, Z., Richardson, J., & Stopa, L. (2019) Psychometric properties of acceptance measures: A systematic review. Journal of Contextual Behavioral Science, 12, 261-277. DOI: 10.1016/j.jcbs.2018.08.006
- Ong, C. W., Lee, E.B., Levin, M.E., & Twohig, M.T. (2019). A review of AAQ variants and other context-specific measures of psychological flexibility. Journal of Contextual Behavioral Science, 12, 329-346. https://doi.org/10.1016/j.jcbs.2019.02.007
- Borgogna, N.C., McDermott, R.C., Berry, A., Lathan, E.C., & Gonzales, J. (2020). A multicultural examination of experiential avoidance: AAQ – II measurement comparisons across Asian American, Black, Latinx, Middle Eastern, and White college students. Journal of Contextual Behavioral Science, 16, 1-8. https://doi.org/10.1016/j.jcbs.2020.01.011
- Aller T.B., Barrett, T., Levin, M.E., Brunson McClain, M. (2022). Measuring psychological flexibility in autistic adults: Examining the validity and reliability of the AAQ-II, BEAQ, and VQ. Journal of Contextual Behavioral Science, 26, 125-133. https://doi.org/10.1016/j.jcbs.2022.09.001
- Ong, C.W., Barthel, A.L., & Hofmann, S.G. (2023). The Relationship Between Psychological Inflexibility and Well-Being in Adults: A Meta-Analysis of the Acceptance and Action Questionnaire. Behavior Therapy. https://doi.org/10.1016/j.beth.2023.05.007
AAQ-II in 30+ Languages
AAQ-II in 30+ Languages CommunityAAQ-II in Arabic
AAQ-II in ArabicAAQ II, 7 item, with scoring. Courtsey of Belal Mustafa.
References:
Hemaid, Fairouz & El-Astal, Sofián & Cangas, Adolfo & Navarro, Noelia & Aguilar-Parra, Jose & Alsaqqa, Ayah & Saqer, Ayah. (2017). PSYCHOMETRIC PROPERTIES OF THE PALESTINIAN VERSION OF THE ACCEPTANCE AND ACTION QUESTIONNAIRE-II (AAQ-II) APPLIED IN THE GAZA STRIP. International Journal of Psycho-Educational Sciences, 5(3), 52-59.
Bougueffa, I. (2020) فعالية العلاج بالتقبل والإلتزام في التخفيف من أعراض الوسواس القهري [The effectiveness of acceptance and commitment therapy in relieving OCD symptoms]. Dissertation, University of Batna. The AAQ-II Arabic version is in the appendix. Retrieved from http://dspace.univ-batna.dz/handle/123456789/1210
AAQ-II in Chinese
AAQ-II in Chinese王小龙, 曹静, 安静, 丁万兵, 索玉兰, 苏华, 李燕, 祝卓宏, 汤永隆 (2015). 中文接纳与行动问卷第二版(AAQ-II)与认知融合问卷(CFQ)在回族和哈萨克族青少年中的信效度检验. 心理学进展, 5(11), 695-701. [Wang Xiaolong, Cao Jing, Jing Jing, Ding Wanbing, Suo Yulan, Su Hua, Li Yan, Zhu Zhuohong, Tang Yonglong (2015). Chinese Acceptance and Action Questionnaire Second Edition (AAQ-II) and Cognitive Fusion Questionnaire (CFQ ) in Hui and Kazak adolescents. Advances in Psychology, 5(11) , 695-701.] http://dx.doi.org/10.12677/AP.2015.511090
Chun-Qing Zhang, Pak-Kwong Chung, Gangyan Si & Jing Dong Liu (2014). Psychometric Properties of the Acceptance and Action Questionnaire–II for Chinese College Students and Elite Chinese Athletes. Measurement and Evaluation in Counseling and Development, 47(4), 256-270. DOI: 10.1177/0748175614538064
CAO Jing, JI Yang, & ZHU Zhuo-Hong (2013). Reliability and validity of the Chinese version of the Acceptance and Action Questionnaire-Second Edition(AAQ-Ⅱ)in college students. Chinese Mental Health Journal, 11, 873-877.
Chang, W.H., Chi, L., Lin, SH. et al. (2017). Psychometric Properties of the Acceptance and Action Questionnaire – II for Taiwanese College Students and Elite Athletes. Curr Psychol 36, 147–156. https://doi.org/10.1007/s12144-015-9395-x
AAQ-II in Croatian
AAQ-II in CroatianŠego, A. (2022). Mentalno zdravlje zdravstvenih djelatnika u vrijeme pandemije COVID–19. [Mental health of healthcare workers in the COVID-19 pandemic]. Thesis: Sveučilište u Splitu, Medicinski fakultet [University of Split, School of Medicine]. https://urn.nsk.hr/urn:nbn:hr:171:198025
AAQ-II in Czech
AAQ-II in CzechPtáček, Martin. (2022). Assessing Effectiveness of the Mindfulness-Acceptance-Commitment Approach in Sport. Thesis: Masarykova Univerzita. Retrieved from https://is.muni.cz/th/qyx1b/ The Czech version of AAQ-II is in the Appendix.
AAQ-II in Danish
AAQ-II in DanishHoffmann, D. Halsboe, L., Eilenberg, T., Jensen, J.S., & Frostholm, L. (2014) A pilot study of processes of change in group-based acceptance and commitment therapy for health anxiety. Journal of Contextual Behavioral Science, 3(3), 189-195. https://doi.org/10.1016/j.jcbs.2014.04.004
AAQ-II in Danish. Updated, 31/8/2015. Login to see attachment
AAQ-II in Dutch
AAQ-II in DutchAAQ-II translated in Dutch. Login to see the attachments.
References:
Fledderus, M., Oude Voshaar, M. A. H., ten Klooster, P. M., & Bohlmeijer, E. T. (2012). Further evaluation of the psychometric properties of the Acceptance and Action Questionnaire–II. Psychological Assessment, 24(4), 925–936. https://doi.org/10.1037/a0028200
Jacobs N, Kleen M, De Groot F, A-Tjak J. (2008) Measuring experiential avoidance. Dutch translation of the Acceptance and Action Questionnaire-II (AAQ-II) [in Dutch]. Gedragstherapie, 41, 349–361.
AAQ-II in Finnish
AAQ-II in FinnishLappalainen, P., Keinonen, K., Pakkala, I., Lappalainen, R., & Nikander, R. (2021). The role of thought suppression and psychological inflexibility in older family caregivers’ psychological symptoms and quality of life. Journal of Contextual Behavioral Science, 20, 129-136. https://doi.org/10.1016/j.jcbs.2021.04.005
(Login to your ACBS account to see the attachment)
AAQ-II in French
AAQ-II in FrenchVersion française de l'AAQ-II dans la Revue Européenne de Psychologie Appliquée.
Monestès, JL., Villatte, M., Mouras, H., Loas, G., & Bond, F. (2009). Traduction et validation française du questionnaire d'acceptation et d'action (AAQ-II). European Review of Applied Psychology, 59, 301-308.
Les résultats indiquent que la version française du questionnaire d'acceptation et d'action-II est fiable et valide. Elle peut donc être utilisée en recherche comme en clinique. [French version of AAQ-II in European Review of Applied Psychology; Abstract below)]
Résumé: L'évitement d'expériences psychologiques douloureuses a été choisi comme cible privilégiée par plusieurs nouvelles approches thérapeutiques issues des thérapies comportementales et cognitives. La tentative de suppression des événements psychologiques désagréables conduit à une perte de la flexibilité psychologique fortement corrélée avec un nombre important et varié de troubles psychologiques. Ces nouvelles approches thérapeutiques tentent d'accroître l'acceptation afin de lutter contre cette rigidité psychologique. Parmi ces approches, la thérapie d'acceptation et d'engagement (ACT) évalue la flexibilité psychologique au moyen du questionnaire d'acceptation et d'action (AAQ-II), qui présente de bonnes propriétés psychométriques. Une version française de l'AAQ-II est ici évaluée sur un groupe de 210 sujets témoins et de 118 patients souffrant de troubles anxieux ou dépressifs. La version française de l'AAQ-II présente une bonne consistance interne. Sa validité concourante comme sa validité de construit semblent solides. Le questionnaire est fiable dans une évaluation en test-retest. La structure factorielle à un facteur de la version francophone de l'AAQ-II est la même que celle de la version originale. Ces résultats assurent une utilisation de la version française de l'AAQ-II en recherche comme en pratique clinique.
[FRENCH TRANSLATION AND VALIDATION OF THE ACCEPTANCE & ACTION QUESTIONNAIRE (AAQ-II)
Keywords: Acceptance & action questionnaire (AAQ-II), Acceptance and commitment therapy, Psychological flexibility
Abstract: Avoidance of painful psychological experience has been chosen as the prime target by several new therapeutic approaches derived from cognitive and behavioral therapies. Attempts to suppress unpleasant emotional events lead to a loss of psychological flexibility strongly correlated with a significant number and variety of psychological disorders. These new therapeutic approaches attempt to increase acceptance in order to decrease this psychological rigidity. Among these approaches, Acceptance and Commitment Therapy (ACT) measures psychological flexibility by mean of Acceptance and Action Questionnaire (AAQ-II), which presents good psychometric properties. A French version of the AAQ-II was evaluated in a group of 210 control subjects and 118 patients with anxiety disorders or depression. The French version of the AAQ-II presents good internal consistency (Cronbach's alpha: 0.76-0.82). Its concurrent validity and construct validity appear strong. The questionnaire is reliable in test-retest evaluation. The one-factor structure of the French version of the AAQ-II reproduces the structure of the original version. These results ensure the use of the French version of the AAQ-II in research as well as in clinical practice.]
AAQ-II in Georgian
AAQ-II in GeorgianNino Gogichadze, Teona Lodia, Nata Meparishvili, & Jodi Polaha (2017) The AAQ-II Translation to Georgian: A Preliminary Validation Study. Poster presented at ACBS Annual World Conference 15
AAQ-II in German
AAQ-II in GermanHoyer, J. & Gloster, A.T. (2013) Psychologische Flexibilität messen: Der Fragebogen zu Akzeptanz und Handeln II. Verhaltenstherapie, 23, 42–44.
Gloster, A., Klotsche, J., Chaker, S., Hummel, K.V., & Hoyer, J. (2011). Assessing psychological flexibility: what does it add above and beyond existing constructs? Psychological assessment, 23(4), 970-82 .
AAQ-II in Greek
AAQ-II in GreekKarekla, M. & Michaelides, M.P. (2017) Validation and invariance testing of the Greek adaptation of the Acceptance and Action Questionnaire -II across clinical vs. nonclinical samples and sexes. Journal of Contextual Behavioral Science, 6(1), 119-124. https://doi.org/10.1016/j.jcbs.2016.11.006
AAQ-II in HINDI
AAQ-II in HINDITyagi, A. & Agarwal, A. (2021). Validation of the Factor Structure of Acceptance and Action Questionnaire-II (AAQ-II) in the Indian Context. Turkish Online Journal of Qualitative Inquiry, 12(7), 10033-10043.
See attachment for translation by Sayma Jameel & Dr M Manjula, National Institute of Mental Health and Neuro Sciences, Bengaluru, Karnataka, India
AAQ-II in Hebrew
AAQ-II in HebrewHebrew translations of the AAQ II is below.
AAQ II
Rabbi Dov Ben-Yaacov BA. LLB.PgD-Psychiatry
MSc Psychiatry candidate, Cardiff Medical School
Cardiff University, Cardiff, Wales, UK
AAQ-II in Hungarian
AAQ-II in HungarianBalazsi, R., Pentek, I., Vargha, J., & Szabo, K. (2019). The investigation of the factor structure, construct validity and gender related differences of the Hungarian version of the Acceptance and Action Questionnaire-II: A latent mean difference approach. Journal of Evidence-Based Psychotherapies, 19(1), 73-89. DOI: 10.24193/jebp.2019.1.5
Eisenbeck, N., & Szabó-Bartha, A. (2018). Validation of the Hungarian version of the Acceptance and Action Questionnaire-II (AAQ-II). Journal of Contextual Behavioral Science, 9, 80-87. https://doi.org/10.1016/j.jcbs.2018.07.007
See attachments for AAQ-II in Hungarian.
Please contact Krizstina-Gabriella Szabo (krisztinagabriella.szabo@gmail.com) for additional information.
AAQ-II in Indonesian
AAQ-II in IndonesianNurmalita Sari, Margaretha Sih Setija Utami, Esthy Rahayu (2022). The Effectiveness of Acceptance and Commitment Therapy (ACT) for Reducing Depression in Post-Stroke Patients. Philanthropy: Journal of Psychology, 6(1), 13 – 31. Retrieved from https://journals.usm.ac.id/index.php/philanthropy/article/view/4681
AAQ-II in Italian
AAQ-II in ItalianPennato, T., Berrocal, C., Bernini, O. et al. (2013) Italian Version of the Acceptance and Action Questionnaire-II (AAQ-II): Dimensionality, Reliability, Convergent and Criterion Validity. J Psychopathol Behav Assess, 35, 552–563 (2013). https://doi.org/10.1007/s10862-013-9355-4 The Italian AAQ-II items are in the Appendix Table 8.
AAQ-II in Japanese
AAQ-II in JapaneseAAQ-II translated in Japanese. Naoko Kishita, Tetsuya Yamamoto, & Hironori Shimada Author contact information: Naoko Kishita Graduate School of Human Sciences, Waseda University, Japan sun_village@suou.waseda.jp
Citations
7 items AAQ-II: Daiki Shima, Mika Yanagihara, Satoshi Kawai, Hiroaki Kumano (2013) Japanese version of Acceptance and Action Questionnaire-II 7-item version. Proceedings of the 77th Annual Meeting of the Japanese Psychological Association.
10 items AAQ-II: Naoko Kinoshita, Tetsuya Yamamoto, Hironori Shimada (2008). Attempt to create Japanese version of Acceptance and Action Questionnaire-II Proceedings of the 21st Annual Meeting of the Japanese Society of Health Psychology, 46.
AAQ-II in Korean
AAQ-II in KoreanHeo, J.H., Choi, M.S., & Jin, H.J. (2009). Study on the reliability and validity of Korean translated Acceptance-Action Questionnaire-II. Journal of the Korean Psychological Association: Counseling and Psychotherapy, 21(4), 861–878. www.kci.go.kr
AAQ-II in Latvian
AAQ-II in LatvianSadauska, I. & Koļesovs, A. (2021). Validity and Reliability of the Acceptance and Action Questionnaire-II: Latvian Version. Cilvēks, tehnoloģijas un izglītības kvalitāte, 2021[Human, Technologies and Quality of Education, 2021], 71-82. https://doi.org/10.22364/htqe.2021
AAQ-II in Malay
AAQ-II in MalayReferences:
Mohd Bahar, F. H., Mohd Kassim, M. A., Pang, N. T. P., Koh, E. B. Y., Kamu, A., & Ho, C. M. (2022). Malay Version of Acceptance and Action Questionnaire-II (AAQ-II): A Reliability and Validity Analysis in Non-Clinical Samples. IIUM Medical Journal Malaysia, 21(3). https://doi.org/10.31436/imjm.v21i3.1888
Shari, N. I., Zainal, N. Z., Guan, N. C., Ahmad Sabki, Z., & Yahaya, N. A. (2019). Psychometric properties of the acceptance and action questionnaire (AAQ II) Malay version in cancer patients. PloS one, 14(2), e0212788. https://doi.org/10.1371/journal.pone.0212788 The Malay Translation is in Appendix 1.
AAQ-II in Norwegian
AAQ-II in NorwegianTranslated AAQ-II in Norwegian. Norsk konsensusversjon (backtranslated), mars 2009 - og revidert i2011 henhold til engelskspråklig validering. Forhåpentligvis vil det gjøres en valideringsstudie av den i nærmeste fremtid. Denne versjonen er utarbeidet av (i alfabetisk rekkefølge): Roar Fosse PhD Børge Holden dr.philos. Didrik Heggdal Psykologspesialist Steffen Holthe Psykolog Trym Nordstrand Jacobsen MA. Ayna B. Johansen PhD Lars Mariero Med.Stud. (for spørsmål kan Trym Nordstrand Jacobsen nåes på trym_n_jacobsen@yahoo.no)
Tom Østergaard, Tobias Lundgren, Robert D. Zettle, Nils Inge Landrø, Vegard Øksendal Haaland (2020) Norwegian Acceptance and Action Questionnaire (NAAQ): A psychometric evaluation. Journal of Contextual Behavioral Science, 15, 103-109. DOI: 10.1016/j.jcbs.2019.12.002
The Acceptance and Action Questionnaire (AAQ-II) aims to measure psychological flexibility (PF), described as the ability to act according to chosen values while consciously being in contact with present moment experiences that might function as obstacles. To date, the psychometric properties of a Norwegian translated version of the AAQ-II (NAAQ) have not been published, thus limiting the confidence of findings based on its use with Norwegian samples. The current study sought to address this omission by evaluating the psychometric properties of the NAAQ in a clinical sample (N = 163) with a history of major depressive disorder and residual symptoms of depression. A confirmatory factor analysis supported a unidimensional structure of the scale with good internal (α = 0.87) and satisfactory levels of concurrent and convergent validity. Incremental validity beyond two measures of value-based living was found in predicting depression, anxiety, and three of four domains reflective of quality of life. The overall results support the use of the NAAQ in both research and clinical practice with Norwegian samples.
Børge Strømgren, Stian Orm Jon A. Løkke (2021) Psychometric Properties of the Norwegian Acceptance and Action Questionnaire in a Non-clinical Sample. International journal of psychology and psychological therapy, 21(2), 199-206.
AAQ-II in Persian
AAQ-II in PersianAbasi, E., Fti, L., Molodi, R., Zarabi, H. (2013). Psychometric properties of Persian Version of Acceptance and Action Questionnaire –II. Journal of Psychological Models and Methods, 3(10), 65-80.
Nezamaddin Ghasemi, Mehrdad Kalantari, Karim Asghari, Hossaein Molavi (2014) Factor Structure, Validity and Reliability of the Persian version of the Acceptance and Action Questionnaire (AAQ-II-7). International Journal of Education and Research, 2(9), 85-96.
AAQ-II translated into Farsi courtesy of Dr. Ali Sahebi. Please contact asahebi@gmail.com for more information. See attached file.
AAQ-II in Polish
AAQ-II in PolishKleszcz, Bartosz & Dudek, Joanna & Białaszek, Wojciech & Ostaszewski, Pawel & Bond, Frank. (2018). Właściwości psychometryczne polskiej wersji Kwestionariusza Akceptacji i Działania (AAQ-II). Studia Psychologiczne, 1, 1-20.
Polski. Oto strona zawierająca Acceptance and Action Questionnaire-II, mierzący elastyczność psychologiczną. Dostępne są dwie wersje - męska i żeńska. Pełne dane dostępne będą po opublikowaniu wyników. Test jest darmowy do użytku w ramach interwencji psychologicznych i badań naukowych. W razie pytań wyślij maila do bkleszcz@gmail.com
English. This is the page containing the Acceptance and Action Questionnaire-II, measuring psychological flexibility. Two versions are available - male and female. Full data will be available after publishing. The test is free for use in psychological intervetions and research. Should you have any questions please send a mail to bkleszcz@gmail.com
AAQ-II in Portuguese
AAQ-II in PortugueseAAQ-II translated in Portuguese. (login to your ACBS account to see attachment)
References:
Pinto-Gouveia, J., Gregório, S., Dinis, A., & Xavier, A. (2012). Experiential Avoidance in Clinical and Non-Clinical Samples: AAQ-II Portuguese Version. International Journal of Psychology and Psychological Therapy, 12(2), 139-156.
Barbosa, L.Martins. & Murta, S. G. (2015). Propriedades psicométricas iniciais do Acceptance and Action Questionnaire - II - versão brasileira. Psico-USF, 20(1), 75-85. https://doi.org/10.1590/1413-82712015200107
Berta-Otero, T., Barceló-Soler, A., Montero-Marin, J., Maloney, S., Pérez-Aranda, A., López-Montoyo, A., Salvo, V., Sussumu, M., García-Campayo, J., & Demarzo, M. (2023). Experiential Avoidance in Primary Care Providers: Psychometric Properties of the Brazilian “Acceptance and Action Questionnaire” (AAQ-II) and Its Criterion Validity on Mood Disorder-Related Psychological Distress. International Journal of Environmental Research and Public Health, 20(1), 225. https://doi.org/10.3390/ijerph20010225
AAQ-II in Romanian
AAQ-II in RomanianSzabó, K.G., Vargha, J.L., Balazsi, R., Bartalus, J., & Bogdan, V. (2011) MEASURING PSYCHOLOGICAL FLEXIBILITY: PRELIMINARY DATA ON THE PSYCHOMETRIC PROPERTIES OF THE ROMANIAN VERSION OF THE ACCEPTANCE AND ACTION QUESTIONNAIRE (AAQ-II). Journal of Cognitive and Behavioral Psychotherapies, Cluj-Napoca, 11, (1), 67-82.
Preliminary data regarding the psychometric properties of the Romanian AAQ-II:
The calculated Cronbach’s Alpha’s value was .80 for the 10-item AAQ-II, and .84 for the 7-item AAQ-II (n = 350, 145 males).
A full description of the psychometric properties is described in the attached documents in English and Romanian. Please contact Krizstina-Gabriella Szabo (krisztinagabriella.szabo@gmail.com) for additional information.
AAQ-II in Russian
AAQ-II in RussianAAQ-II
Опросник Принятия И Дейcтвий -II
References:
Yasin, M.I. (2022). Русскоязычная адаптация методик для диагностики принятия и избегания опыта [Russian-language adaptation of methods for diagnosing acceptance and avoidance of experience]. Современная зарубежная психология [Journal of Modern Foreign Psychology], 11(2), 113–121. https://doi.org/10.17759/jmfp.2022110210
AAQ-II in Serbian
AAQ-II in SerbianDragan Žuljević, Nikolija Rakočević, & Igor Krnetić (2020). Testing the Model of Psychological Flexibility in the Serbian Cultural Context: The Psychometric Properties of the Acceptance and Action Questionnaire. Psihologija, 53 (2), 161-181. https://doi.org/10.2298/PSI191015006Z
Translated to Serbian by Dr Dragan Zuljevic, Dr Igor Krnetic and Nikolija Rakocevic.
Please contact drzuljevic@gmail.com for more information
AAQ-II in Spanish
AAQ-II in SpanishReferences
- Patrón Espinosa, F. (2010). La evitacion experiencial y su medicion por medio del AAQ-II. Enseñanza e Investigación en Psicología, 15(1), 5-19. At the end of the article is the measure
- Ruiz, F.J., Langer Herrera, A.I., Luciano, C., Cangas, A.J. & Beltrán, I. (2013). Measuring experiential avoidance and psychological infl exibility: The Spanish version of the Acceptance and Action Questionnaire - II. Psicothema, 25, 123-129. DOI: 10.7334/psicothema2011.239
- Paladines-Costa, B., López-Guerra, V., Ruisoto, P., Vaca-Gallegos, S., & Cacho, R. (2021). Psychometric Properties and Factor Structure of the Spanish Version of the Acceptance and Action Questionnaire-II (AAQ-II) in Ecuador. International journal of environmental research and public health, 18(6), 2944. https://doi.org/10.3390/ijerph18062944
AAQ-II Adaptación Luciano, Ruiz, 2007 (Login to your ACBS account to see attachments)
AAQ-II in Swedish
AAQ-II in SwedishHayes et al utvecklade den första versionen av AAQ med 10 frågor. Den har senare översatts till svenska och förkortat till 6 frågor av Tobias Lundgren och Thomas Parling vid Uppsala Universitet. Du hittar instrumentet här.
Referenser:
[1] Nilsson, P. (2021) Psykologisk Inflexibilitet och Kognitiv Fusion hos Vuxna med Autism: En Studie om Acceptance and Commitment Therapy. Mituniversitetet, thesis. Swedish 7 item AAQ-II is in Bilaga 3.1. Retrieved from https://www.diva-portal.org/smash/get/diva2:1566478/FULLTEXT01.pdf
[2] Thorsell Cederberg, J., Sandra Weineland, S., Dahl,J., & Ljungman, G. (2018). Validation of the Swedish Acceptance and Action Questionnaire (SAAQ) for parents of children with cancer. Journal of Contextual Behavioral Science, 10, 50-54. https://doi.org/10.1016/j.jcbs.2018.08.008
[3] Tobias Lundgren & Thomas Parling (2017): Swedish Acceptance and Action Questionnaire (SAAQ): a psychometric evaluation, Cognitive Behaviour Therapy. Du kan läsa artikeln i fullängd här: http://dx.doi.org/10.1080/16506073.2016.1250228
[4] Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. C., Guenole, N., Orcutt, H. K., Waltz, T. and Zettle, R. D. (2011). Preliminary psychometric properties of the Acceptance and Action Questionnaire – II: A revised measure of psychological flexibility and acceptance. Behavior Therapy, 42, 676-688.
[5] Hayes S.C., Strosahl K.D., Wilson K.G., Bissett R.T., Pistorello J., Toarmino D., Polusny M.A., Dykstra T.A., Batten S.V., Bergan J., Stewart S.H., Zvolensky M.J., Eifert G.H., Bond F.W., Forsyth J.P., Karekla M, McCurry SM. Measuring experiential avoidance: a preliminary test of a working model. The Psychological Record 2004;54:553–78.
[6] Otto, N. (2010). Den svenska versionen av Acceptance and Action Questionnaire. En psykometrisk utvärdering. Opublicerad psykologexamensuppsats, Institutionen för psykologi, Uppsala universitet, Uppsala.
AAQ-II in Tamil
AAQ-II in TamilDr. Veera Balaji Kumar has shared his Tamil translation of AAQ-II. Therapists working with Tamil speaking clients can utilize this measure.
Proviso: Although this translation was cross-checked by a language expert and found workable in Veera's practice, it has not been psychometrically tested for accuracy.
AAQ-II in Thai
AAQ-II in ThaiSumalrot, T., Phannajit, N., & Phattharayuttawat, S. (2022). Psychometric Properties of Scales for Assessing Experiential Avoidance. Siriraj Medical Journal, 74(11), 760–768. https://doi.org/10.33192/Smj.2022.90
Sucheera Phattrayuttrawat, Thanayot Sumalrot & Naphol Phannajit (2019) A STUDY OF PSYCHOMETRIC PROPERTIES OF SELF-RATING SCALES FOR ASSESSING EXPERIENTIAL AVOIDANCE. Proceeding of Graduate Research Forum 2019 An Academic Conference for Graduate Student.
Pimpanit Condee, Nattasuda Taephant Kullaya Pisitsungkagarn (2017) Development of a Thai version of the Acceptance Scale and Preliminary Psychological Properties for Individuals after Leukemia Treatment. Journal of the Royal Thai Army Nurses, 18 (suppl.1),174-80. Available from: https://he01.tci-thaijo.org/index.php/JRTAN/article /view/90119 The Thai translation of the AAQ-II items is in the table 1.
AAQ-II in Turkish
AAQ-II in TurkishFatih Yavuz, Sevinc Ulusoy, Mehtap Iskin, Fatma Betul Esen, Huseyin Sehid Burhan, Mehmet Emrah Karadere & Nuran Yavuz (2016) Turkish Version of Acceptance and Action Questionnaire-II (AAQ-II): A reliability and Validity Analysis in Clinical and Non-Clinical Samples. Klinik Psikofarmakoloji Bülteni-Bulletin of Clinical Psychopharmacology, 26(4), 397-408, http://doi.org/10.5455/bcp.20160223124107
Meunier, B., Atmaca, S., Ayranci, E., Gökdemir, B. P., Uyar, T., & Bastug, G. (2014). Psychometric properties of the Turkish version of the acceptance and action questionnaire-II (AAQ-II). Journal of Evidence-Based Psychotherapies, 14(2), 179.
Fatih Yavuz, M.D., Mehtap Iskin, Psyc, Sevinc Ulusoy, M.D., Betul Esen, M.D., Huseyin Sehid Burhan, M.D. (2014) Turkish Version of AAQ-II: Preliminary Analysis of Reliability and Validity. Poster presented at the ACBS Annual World Conference 12.
KABUL VE EYLEM FORMU-2 (See attachment)
AAQ-II in Ukranian
AAQ-II in UkranianShiroka, A.A. & Mykolaychuk, M.I. (2021). АДАПТАЦІЯ УКРАЇНОМОВНОЇ ВЕРСІЇ ОПИТУВАЛЬНИКА ПРИЙНЯТТЯ ТА ДІЇ (AAQ-II) НА НОРМАТИВНІЙ ТА СУБКЛІНІЧНІЙ ГРУПАХ ДОСЛІДЖУВАНИХ [ADAPTATION OF THE UKRAINIAN-VERSION VERSION OF THE QUESTIONNAIRE OF ACCEPTANCE AND ACTION (AAQ-II) ON NORMATIVE AND SUBCLINICAL GROUPS OF RESEARCHES]. Scientific Bulletin of KSU Series Psychological Sciences, 2021(No. 3), 101-112. https://doi.org/10.32999/ksu2312-3206/2021-3-14 The AAQ-II Items Ukraianian translation is in Table 4.
AAQ-II in Urdu
AAQ-II in UrduAAQ-II in Urdu Translated by Sumayya Sajjad <sumayyasajjad75@yahoo.com>
Centre for Clinical Psychology
University of the Punjab, Lahore, Pakistan
Acceptance and Action Questionnaire II-Urdu Translated by Rabia Khawar, Ph.D - rabiakhawar@gcuf.edu.pk
Associate Professor
Chairperson Department of Applied Psychology
GC University Faisalabad
AAQ in languages other than English
AAQ in languages other than English CommunityAAQ in Albanian
AAQ in AlbanianMorina, N. (2007) Der Zusammenhang zwischen Erlebnisvermeidung und posttraumatischen Belastungssymptomen nach Kriegstraumatisierung - eine Kurzmitteilung [The Relationship Between Experiential Avoidance and Posttraumatic Symptoms Following War Trauma - A Brief Report]. Psychotherapie Psychosomatik Medizinische Psychologie, 58, 69-71. http://doi.org/10.1055/s-2007-971010
AAQ in Chinese
AAQ in ChineseAAQ translated in Chinese.
Author contact information:
Ai-Ti Tseng
Clinical psychologist, Taiwan
emily0507cs@yahoo.com.tw
AAQ in French
AAQ in French adminAAQ in German
AAQ in GermanAAQ (22 item) German
AAQ (22 item) GermanGerman 22-item AAQ.
AAQ (9 item) German
AAQ (9 item) GermanThis German version of the AAQ was used in a study by these authors
AAQ in Hebrew
AAQ in HebrewHebrew translations of the AAQ 10 and 7-item scales are below.
AAQ 10-item scale:
Liad Bareket-Bojmel
Department of Behavioral Sciences, Ben-Gurion University
liadbar@bgu.ac.il
AAQ II 7-item scale:
Rabbi Dov Ben-Yaacov BA. LLB. PgD-Psychiatry
MSc Psychiatry candidate, Cardiff Medical School
Cardiff University, Cardiff, Wales, UK
AAQ in Korean
AAQ in Korean16 question AAQ in Korean. Courtsey of HEO, Jaehong.
AAQ in Spanish
AAQ in SpanishSpanish version of the AAQ.
References:
Barraca, J. (2004). Spanish Adaptation of the Acceptance and Action Questionnaire (AAQ). International Journal of Psychology and Psychological Therapy, 4, (3), 505-515.
Ruiz, F.J., Langer, A.I., Luciano, C., Cangas, A.J., & Beltrán, I. (2013). Midiendo la evitacion experiencial y la inflexibilidad psicologica: version espanola del Cuestionario de Aceptacion y Accion-II [Measuring experiential avoidance and psychological inflexibility: the Spanish translation of the Acceptance and Action Questionnaire]. Psicothema, 25,123-129. http://doi.org/10.7334/psicothema2011.239
AAQ -Spanish excel version
AAQ -Spanish excel versionAttached there is an excel version of the Spanish AAQ (Barraca Mairal, 2006), with automatic correction.
AAQ in Swedish
AAQ in SwedishThe 22 item version (the one you can score all vaidated ways) of the AAQ-I in Swedish. Translated by Rikard Calmbro and Henrik Torneskog. The translators can be reached at calmbro@hotmail.com.
Brief Experiential Avoidance Questionnaire (BEAQ)
Brief Experiential Avoidance Questionnaire (BEAQ)Gámez, W., Chmielewski, M., Kotov, R., Ruggero, C., Suzuki, N., & Watson, D. (2014). The Brief Experiential Avoidance Questionnaire: Development and initial validation. Psychological Assessment, 26(1), 35–45. https://doi.org/10.1037/a0034473
Vázquez-Morejón, R. et al. (2019). Validation of a Spanish version of the Brief Experiential Avoidance Questionnaire (BEAQ) in clinical population. Psicothema, 31(3), 335-340. DOI: 10.7334/psicothema2019.60 You can find the BEAQ in the appendix.
Ong, C.W., Pierce, B.G., Petersen, J.M., Barney, J.L., Fruge, J.E., Levin, M.E., & Twohig, M.P. (2020). A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance. Journal of Contextual Behavioral Science, 18, 34-47. https://doi.org/10.1016/j.jcbs.2020.08.007
Aller, T.B., Barrett, T., Levin, M.E., McClain, M.B. (2022). Measuring psychological flexibility in autistic adults: Examining the validity and reliability of the AAQ-II, BEAQ, and VQ. Journal of Contextual Behavioral Science, 26, 125-133. DOI: 10.1016/j.jcbs.2022.09.001
BEAQ - Chinese Validation
BEAQ - Chinese ValidationCao, H. et al (2021) Chinese validation of the Brief Experiential Avoidance Questionnaire (BEAQ) in college students. Journal of Contextual Behavioral Science, 19, 79-85. https://doi.org/10.1016/j.jcbs.2021.01.004 The BEAQ translation in Simplified Chinese is in the Appendix.
Lo, H.H.M., Powell, C.L.Y.M., Chan, S.H.W. et al. (2023). Validating an Adapted Version of the Brief Experiential Avoidance Questionnaire in Hong Kong Chinese. Journal of Psychopathology and Behavioral Assessment, 45, 207–220. https://doi.org/10.1007/s10862-022-10020-w
BEAQ - Czech
BEAQ - CzechPetříková, K. (2021). Atributy acceptance and commitment therapy (ACT) v kontextu syndromu vyhoření u studentů medicíny. Thesis: Masarykova Univerzita. Retrieved from https://is.muni.cz/th/ww25y/ The Czech version of BEAQ is in the Appendix.
BEAQ - German Validation
BEAQ - German ValidationReferences:
Schaeuffele, C., Knaevelsrud, C., Renneberg, B., & Boettcher, J. (2022). Psychometric Properties of the German Brief Experiential Avoidance Questionnaire (BEAQ). Assessment, 29(7), 1406-1421. https://doi.org/10.1177/10731911211010955
BEAQ - Japanese
BEAQ - JapaneseSAKAGUCHI, R., SEGUCHI, A., & MITAMURA, T. (2023). 日本語版 Brief Experiential Avoidance Questionnaire BEAQ) の開発 [Developing the Japanese version of the Brief Experiential Avoidance Questionnaire]. RITSUMEIKAN JOURNAL OF HUMAN SCIENCES, 47, 1-11.
BEAQ - Korean
BEAQ - KoreanLee Ju-Yeon, You Sung-Eun (2017) 한국판 다차원적 경험회피 척도(K-MEAQ)의 타당화 및 단축형(K-MEAQ-24) 개발 [Validation of the Korean Version of the Multidimensional Experiential Avoidance Questionnaire(K-MEAQ) and Development of a Brief Form(K-MEAQ-24)]. Cognitive Behavior Therapy in Korea, 17, 2, 181 - 208.
BEAQ - Spanish Validation
BEAQ - Spanish ValidationVázquez-Morejón, R. et al. (2019). Validation of a Spanish version of the Brief Experiential Avoidance Questionnaire (BEAQ) in clinical population. Psicothema, 31(3), 335-340. DOI: 10.7334/psicothema2019.60
The BEAQ in Spanish and English are included in the appendix of this article.
Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT)
Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT)The CompACT was developed as a general measure of psychological flexibility (and constituent sub-processes) as conceptualized within the ACT model. The development and initial validation of the measure is reported in the manuscript attached below, which has been published in the Journal of Contextual Behavioral Science (accessible here).
The CompACT is free to use for clinical and research purposes: we have attached the CompACT response form and a scoring calculator below. We hope it will prove to be a useful measure, building on the promise of our initial findings. There are also now CompACT short form versions.
Citations for CompACT:
Francis, A.W., Dawson, D.L., & Golijani-Moghaddam, N. (2016) The development and validation of the Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT). Journal of Contextual Behavioral Science, 5(3), 134-145. https://doi.org/10.1016/j.jcbs.2016.05.003.
Ong, C.W., Pierce, B.G., Petersen, J.M., Barney, J.L., Fruge, J.E., Levin, M.E., & Twohig, M.P. (2020). A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance. Journal of Contextual Behavioral Science, 18, 34-47. https://doi.org/10.1016/j.jcbs.2020.08.007
Adamowicz, J.L., Thomas, E.B.K., Hsu, T., Denburg, N.L. & Roche, A.I. (2023). A Preliminary Investigation into the Factor Structure of Two Psychological Flexibility Measures in a Sample of Community-Dwelling Older Adults. Clinical Gerontologist, 46(4), 561-573. DOI: 10.1080/07317115.2022.2131496
Citations for CompACT Short Form Versions:
CompACT-15: Hsu, T., Hoffman, L., & Thomas, E. B. K. (2023). Confirmatory measurement modeling and longitudinal invariance of the CompACT-15: A short-form assessment of psychological flexibility. Psychological Assessment, 35(5), 430–442. https://doi.org/10.1037/pas0001214
CompACT-10: Golijani-Moghaddam, N., Morris, J.L., Bayliss, K., & Dawson, D.L. (2023). The CompACT-10: Development and validation of a Comprehensive assessment of Acceptance and Commitment Therapy processes short-form in representative UK samples. Journal of Contextual Behavioral Science, 29, 59-66. https://doi.org/10.1016/j.jcbs.2023.06.003
CompACT-8: Morris, J., Golijani-Moghaddam, N., & Dawson, D. (2019) Development and validation of a short form of the Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT-SF). DClinPsy thesis, University of Nottingham.
CompACT-8: Dawson, D.L. & Golijani-Moghaddam, N. (2020). COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. Journal of Contextual Behavioral Science, 17, 126-134. DOI: 10.1016/j.jcbs.2020.07.010
CompACT - Chinese
CompACT - ChineseChen, Y., Luo, H., Wang, S., Bai, X., & Zhu, Z. (2023). Preliminary validation of a Chinese version of the comprehensive assessment of acceptance and commitment therapy processes. Current Psychology, 42, 15528–15538. https://doi.org/10.1007/s12144-021-02654-y
CompACT - Czech
CompACT - CzechPtáček, M., & Jelínek, M. (2024). Assessing psychological flexibility: The psychometric properties of the Czech translation of the CompACT questionnaire. Československá psychologie, 68(1), 30–48. https://doi.org/10.51561/cspsych.68.1.30 The CompACT Czech version is available on Open Science Framework: https://osf.io/cwjxq/
CompACT - German
CompACT - GermanGiovannetti, A. M., Pöttgen, J., Anglada, E., Menéndez, R., Hoyer, J., Giordano, A., Pakenham, K. I., et al. (2022). Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes. International Journal of Environmental Research and Public Health, 19(6), 3150. MDPI AG. Retrieved from http://dx.doi.org/10.3390/ijerph19063150
CompACT - Indonesian
CompACT - IndonesianGitta Annisa Vania Suganda & Fitri Ariyanti Abidin (2022). The Comprehensive Assessment of Acceptance and Commitment Treatment Process (Compact): Adaptation of The Indonesian Version. Journal of Educational, Health and Community Psychology, 11(3). Retrieved from www.researchgate.net
CompACT - Italian
CompACT - ItalianGiovannetti, A. M., Pöttgen, J., Anglada, E., Menéndez, R., Hoyer, J., Giordano, A., Pakenham, K. I., et al. (2022). Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes. International Journal of Environmental Research and Public Health, 19(6), 3150. MDPI AG. Retrieved from http://dx.doi.org/10.3390/ijerph19063150<
CompACT - Malay
CompACT - MalayMusa, N., Pang, N.T.P., Kamu, A., Ho, C.M., Waters, C., Berrett, J., Moghaddam, N., & Wider, W. (2022). The Development and Validation of the Comprehensive Assessment of Acceptance and Commitment Therapy Processes (CompACT)—Malay Version. International Journal of Environmental Research and Public Health, 19(15), 9624. DOI: 10.3390/ijerph19159624
CompACT - Persian
CompACT - PersianReferences:
Hajloo, N., Pourabdol, S., Sobhi-Gharamaleki, N., & Beyki, M. (2022). Psychometric Properties of the Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT). Qom University of Medical Science Journal, 15(11). URL: http://journal.muq.ac.ir/article-1-3352-en.html
Soleimani, Z., Shairi, M. (2022). Examination of validity and reliability of the Comprehensive Assessment of Acceptance and Commitment Therapy processes (COMPACT) in non-clinical iranian sampels. Clinical Psychology and Personality, 19(2), 121-137. http://doi.org/10.22070/cpap.2021.3077
CompACT - Portuguese
CompACT - PortugueseReferences
Inês A. Trindade, Nuno B. Ferreira, Ana Laura Mendes, Cláudia Ferreira, Dave Dawson, & Nima Golijani-Moghaddam (2021). Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT): Measure refinement and study of measurement invariance across Portuguese and UK samples. Journal of Contextual Behavioral Science, 21, 30-36. https://doi.org/10.1016/j.jcbs.2021.05.002
Inês A.Trindade, Paula Vagos, Helena Moreira, Daniela V.Fernandes, & IanTyndall (2022). Further validation of the 18-item Portuguese CompACT scale using a multi-sample design: Confirmatory factor analysis and correlates of psychological flexibility. Journal of Contextual Behavioral Science, 25, 1-9. https://doi.org/10.1016/j.jcbs.2022.06.003
CompACT - Romanian Version
CompACT - Romanian VersionCălinici, M. S., & Călinici, T. (2021). COMPREHENSIVE ASSESSMENT OF ACT PROCESSES COMPACT. ROMANIAN ADAPTATION AND SHORT FORM VALIDATION. Journal of Evidence-Based Psychotherapies, 21(2). DOI: 10.24193/jebp.2021.2.19
Submitted by Simona Calinici on January 23, 2021
Completați cu scoruri de la 0 la 6, în funcție de cât de bine vi se potrivesc următoarele afirmații ( 0= deloc, 6= maxim)
1. Pot identifica lucrurile care contează în viață pentru mine și să le urmăresc.
2 r. Unul dintre cele mai importante scopuri ale mele este a evita amintirile dureroase.
3. r Desfășor activități semnificative fără să fiu cu adevărat atent la ele.
4r .Încerc să fiu mereu ocupat ca să nu-mi vină gânduri sau emoții în minte.
5. Acționez în concordanță cu felul cum doresc să-mi desfășor viața.
6r.Sunt atât de prins în gândurile mele că nu pot să fac nici lucrurile pe care doresc cel mai mult să le fac.
7. Fac alegeri în funcție de ce este important pentru mine, chiar dacă este stresant.
8 r Îmi spun că n-ar trebui să am anumite gânduri.
9.r Îmi este greu să rămân concentrat pe ceea ce se întamplă în prezent.
10. Mă comport conform valorilor mele.
11.r Evit situațiile care mi-ar putea produce gânduri, emoții sau senzații neplăcute.
12. r Chiar și când fac lucruri care contează pentru mine, îmi dau seama că le fac fără să fiu atent la ele.
13. Sunt dispus să trăiesc orice gânduri, emoții sau senzații se ivesc, fără să încerc să le schimb sau să mă apăr de ele.
14. Întreprind lucruri care au semnificație pentru mine, chiar dacă mi-e greu.
15.r Mă străduiesc mult să țin la distanță sentimentele supărătoare.
16. r Fac lucruri și sarcini automat, fără să-mi dau seama când le fac.
17. Pot să-mi urmez planurile pe termen lung chiar și atunci când progresul este lent.
18.r Nu fac ceva, chiar dacă e important pentru mine, dacă există riscul de a suferi.
19.r Se pare că funcționez pe pilot automat, fără prea multă atenție la ce fac.
20. Gândurile sunt doar gânduri, ele nu controlează ce fac eu.
21.Valorile mele se reflectă cu adevarat în acțiunile mele (în comportamentul meu).
22. Pot să iau gândurile și emoțiile așa cum vin , fără să încerc să le controlez sau evit.
23. Pot să perseverez în ceva, dacă e important pentru mine.
Traducere și adaptare pentru populația românească Simona Călinici (UMF Iuliu Hațieganu Cluj Napoca, simona.calinici@gmail.com)
CompACT - Spanish
CompACT - SpanishSalvador Reyes-Martín; Mónica Hernández-López; Miguel Rodríguez-Valverde (2021) Spanish adaptation of the Comprehensive Assessment of Acceptance and Commitment Therapy processes (CompACT). Poster presented at ACBS Annual World Conference 19.
Giovannetti, A. M., Pöttgen, J., Anglada, E., Menéndez, R., Hoyer, J., Giordano, A., Pakenham, K. I., et al. (2022). Cross-Country Adaptation of a Psychological Flexibility Measure: The Comprehensive Assessment of Acceptance and Commitment Therapy Processes. International Journal of Environmental Research and Public Health, 19(6), 3150. MDPI AG. Retrieved from http://dx.doi.org/10.3390/ijerph19063150<
CompACT - Swedish
CompACT - SwedishMarie-Louise Möllerberg, Graciela Rovner, Jeanette Melin, & Magnus Johansson. (2021, June 11). CompACT-23 questionnaire, Swedish translation. Zenodo. DOI: 10.5281/zenodo.4925832
The Swedish translation is described and available at: https://doi.org/10.5281/zenodo.4925832
CompACT - Tamil Version
CompACT - Tamil VersionThe original Comprehensive assessment of Acceptance and commitment therapy processes (CompACT) has been tranlsated into Tamil language and is in the process of validation. Researchers can help in the process of assessing the psychometric properties of the translated version.
CompACT-15
CompACT-15A short-form multidimensional measure of psychological flexibility components, including openness to experiences, behavioral awareness, and valued action subscales. Attached is the scale and an Excel coding sheet for ease of use.
Hsu, T., Hoffman, L., & Thomas, E. B. K. (2023). Confirmatory measurement modeling and longitudinal invariance of the CompACT-15: A short-form assessment of psychological flexibility. Psychological Assessment, 35(5), 430–442. DOI: 10.1037/pas0001214
Here is a link to the publicly available manuscript: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10101904/
The manuscript reports on CFA and IFA latent variable measurement models that supported a 15-item short-form. The three-factor structure demonstrated good fit. Acceptable reliability was observed across the three factors. Moreover, the results indicated measurement equivalence of the items to assess latent change over time. Construct validity was also demonstrated.
Many thanks to the CompACT's authors (Ashley W. Francis, David L. Dawson, & Nima Golijani-Moghaddam) for their willingness to allow us to use the scale's items in this work!
Everyday Psychological Inflexibility Checklist (EPIC)
Everyday Psychological Inflexibility Checklist (EPIC)References:
Thompson, M., Bond, F.W., & Lloyd, J. (2019) Preliminary psychometric properties of the Everyday Psychological Inflexibility Checklist. Journal of Contextual Behavioral Science, 12, 243-252. https://doi.org/10.1016/j.jcbs.2018.08.004 The Everyday Psychological Inflexibility Checklist is at the end of the article.
Ong, C,.W., Sheehan, K.G., Haaga, D.A.F. (2023) Measuring ACT in context: Challenges and future directions. Journal of Contextual Behavioral Science, 28, 235-247. https://doi.org/10.1016/j.jcbs.2023.04.005
Flexibility Index Test (FIT-60)
Flexibility Index Test (FIT-60)References:
Batink, T., & Delespaul, P. (2015). Meten van psychologische flexibiliteit – De Flexiibiliteits Index Test (FIT-60). Tijdschrift voor Gedragstherapie, 48(4), 310-332.
Batink, T., Jansen, G., & de Mey, H. (2013). Development of the Flexibility Index Test (FIT-60). Poster presented at ACBS Annual World Conference 11. (See attachment below)
Batink, T., Jansen, G. & De Mey, H.R.A. (2012). De Flexibiliteits Index Test (FIT-60): Een beknopte beschrijving. GZ-Psychologie, 5, 18-21.
The English vesion and Dutch version of the FIT-60 can be found at www.actinactie.nl/flexibiliteits-index-test-fit-60
FIT-60 - Dutch
FIT-60 - DutchBatink, T., & Delespaul, P. (2015). Meten van psychologische flexibiliteit – De Flexiibiliteits Index Test (FIT-60). Tijdschrift voor Gedragstherapie, 48(4), 310-332.
Batink, T., Jansen, G. & De Mey, H.R.A. (2012). De Flexibiliteits Index Test (FIT-60): Een beknopte beschrijving. GZ-Psychologie, 5, 18-21.
The Flexibility Index Test (FIT-60) Dutch version is here https://www.actinactie.nl/flexibiliteits-index-test-fit-60/
Multidimensional Experiential Avoidance Questionnaire (MEAQ)
Multidimensional Experiential Avoidance Questionnaire (MEAQ)Gámez, W., Chmielewski, M., Kotov, R., Ruggero, C., & Watson, D. (2011). Development of a measure of experiential avoidance: The Multidimensional Experiential Avoidance Questionnaire. Psychological Assessment, 23(3), 692–713. https://doi.org/10.1037/a0023242
MEAQ - Dutch
MEAQ - DutchJansen, S., Klundert, N. van de, & Rinia, K. (2016) De drijfveren van experiëntiële vermijding: het verband tussen experiëntiële vermijding, regulatiefocus en actie-oriëntatie [The drivers of experiential avoidance}. Universiteit Utrecht, Thesis. The Multidimensional Experiential Avoidance Questionnaire (Nederlandse vertaling) is in Appendix C.
MEAQ - Korean
MEAQ - KoreanJung, J.-H. (2018). A study on the reliability and validity of the Korean version of the multidimensional experience avoidance questionnaire. Journal of the Korean Contents Association, 18 (1), 517–526. https://doi.org/10.5392/JKCA.2018.18.01.517
MEAQ - Persian
MEAQ - PersianMoradi, A., Barghi Irani, Z., Bagiyan Koulemarz, M., Kariminejad, K., & Zabet, M. (2018). Factor Determination and Psychometric Features of the Multidimensional Experiential Avoidance Questionnaire (MEAQ). Social Cognition, 6(2), 57-82.
URL: http://sc.journals.pnu.ac.ir/article_4422.html?lang=en
MEAQ - Polish
MEAQ - PolishBaran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
See attachments for female and male versions of the MEAQ-30.
MEAQ - Thai
MEAQ - ThaiSumalrot, T., Phannajit, N., & Phattharayuttawat, S. (2022). Psychometric Properties of Scales for Assessing Experiential Avoidance. Siriraj Medical Journal, 74(11), 760–768. https://doi.org/10.33192/Smj.2022.90
Phattrayuttrawat, S., Sumalrot, T. & Phannajit, N. (2019). A STUDY OF PSYCHOMETRIC PROPERTIES OF SELF-RATING SCALES FOR ASSESSING EXPERIENTIAL AVOIDANCE. Proceeding of Graduate Research Forum 2019 An Academic Conference for Graduate Student.
MEAQ - Turkish
MEAQ - TurkishHalil Eksi, et al. (2018) MULTIDIMENSIONAL EXPERIENTIAL AVOIDANCE QUESTIONNAIRE-30: ADAPTATION AND PSYCHOMETRIC PROPERTIES OF THE TURKISH VERSION. ULEAD 2018 Annual Congress: ICRE. The MEAQ Turkish translation is in the article.
Multidimensional Psychological Flexibility Inventory (MPFI)
Multidimensional Psychological Flexibility Inventory (MPFI)GOALS IN DEVELOPING THE MPFI
Dr. Ron Rogge developed the MPFI in collaboration with Dr. Kelly Wilson and Jaci Rolffs. We specifically wanted to create the first scale to comprehensively assess the 6 key dimensions of flexibility and 6 key dimensions of inflexibility from the Hexaflex model.
DEVELOPING THE SCALE
We created an item pool of over 550 items (including 22 of the most widely used scales from the ACT and mindfulness literatures) and gave those items to over 3000 online respondents. We then identified 12 dimensions of flexibility and inflexibility corresponding to the Hexaflex model and selected the 5 most effective items for assessing each dimension with Item Response Theory (IRT) to create the 60-item MPFI.
SCORING
Subscales – To score the MPFI subscales, you assign responses point values from 1 to 6 and then average the responses across the items of each scale so that higher scores reflect higher levels of the dimension being assessed by each set of items.
Global Composites – The averages of the 6 flexibility subscales can be averaged to create a composite representing global flexibility. Similarly, the averages of the 6 inflexibility subscales can be averaged to create a global inflexibility composite.
Shorter Global Composites – The first two items of each of the flexibility subscales can be averaged to create a shorter 12-item global flexibility composite. Similarly, the first 2 items of each of the inflexibility subscales can be averaged to create a shorter 12-item global inflexibility composite.
INTERPRETATION
Normative Information – The research article developing the MPFI (Rolffs, Rogge, & Wilson, 2016; see citation below) presents basic normative data on its subscales (e.g., means and standard deviations by gender). That information will help to place individual scores into a larger context.
Reliable Change – The article also presents Minimal Detectible Change (MDC-95; Stratford, Finch, et al., 1996) estimates for each subscale and for the global composites. These MDC-95 estimates tell researchers and clinicians how many points an individual would need to change on each scale between assessments for that change to be statistically significant. Thus, these MDC95 estimates allow ACT researchers and clinicians to identify clinically significant (i.e., reliable) change groups as suggested by Jacobson and Truax (1991).
Online Interpretative Profiles – The research team is currently piloting an online system (the MindFlex Assessment System - mindflex.org) that not only administers the MPFI (along with some well-validated measures of global functioning) to clients, but also scores the results and provides therapists with standardized flexibility/inflexibility profiles to help inform their work with those clients. In fact, we are currently recruiting therapists for the MindFlex Assessment Project, a research project helping to validate this online service that provides the first ~100 therapists to enroll an opportunity to earn up to $100 for participating (and the first ~300 clients an opportunity to earn up to $80).
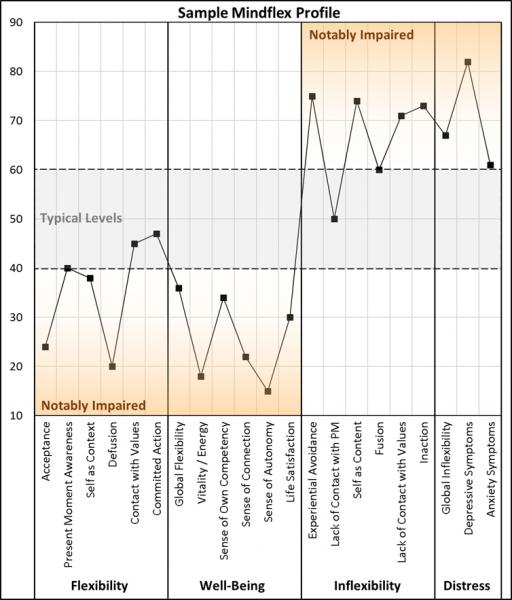
CITATION
If you are using this scale, then you should cite the research article validating it as follows:
Rolffs, J. L., Rogge, R. D., & Wilson, K. G. (2016). Disentangling Components of Flexibility via the Hexaflex Model Development and Validation of the Multidimensional Psychological Flexibility Inventory (MPFI). Assessment, 25(4), 458–482. https://doi.org/10.1177/1073191116645905.
Additional Citations:
Grégoire, S. et al (2020). Validation of the English and French versions of the multidimensional psychological flexibility inventory short form (MPFI-24). Journal of Contextual Behavioral Science, 18, 99-110. https://doi.org/10.1016/j.jcbs.2020.06.004
Barrett, K., O’Connor, M. & McHugh, L. A. (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
MFPI - Italian
MFPI - ItalianLandi, G. et al (2021). Italian Validation of the Italian Multidimensional Psychological Flexibility Inventory (MPFI). Journal of Contextual Behavioral Science, 21, 57-65. https://doi.org/10.1016/j.jcbs.2021.05.007 Italian Translation is in the appendix.
MPFI - Chinese Validation
MPFI - Chinese ValidationLin, Y., Rogge, R.D., Swanson, D.P. (2020). Cross-cultural flexibility: Validation of the traditional Mandarin, simplified Mandarin, and Japanese translations of the Multidimensional Psychological Flexibility Inventory. Journal of Contextual Behavioral Science, 15, 73-84. https://doi.org/10.1016/j.jcbs.2019.11.008 The MPFI Chinese translation is in Appendix A Supplementary data.
(Login into your ACBS account to see the attachments)
MPFI - Japanese
MPFI - JapaneseLin, Y., Rogge, R.D., Swanson, D.P. (2020). Cross-cultural flexibility: Validation of the traditional Mandarin, simplified Mandarin, and Japanese translations of the Multidimensional Psychological Flexibility Inventory. Journal of Contextual Behavioral Science, 15, 73-84. https://doi.org/10.1016/j.jcbs.2019.11.008 The MPFI Japanese translation is in Appendix A Supplementary data.
MPFI - Norwegian
MPFI - NorwegianNorsk versjon kort og lang samt skåringsark tilgjengelig for egen bruk
MPFI - Persian
MPFI - PersianZahra Azadfar, Abbas Abdollahi, Indrajit Patra, Ya-Ping Chang, Tawfeeq Alghazali, Saad Ghazi Talib (2022). The Iranian form of psychometric properties of the Multidimensional Psychological Flexibility Inventory. Psicologia: Reflexão e Crítica, 35. https://doi.org/10.1186/s41155-022-00236-w
.
MPFI - Portuguese
MPFI - PortuguesePereira, C., Cunha, M., Massano-Cardoso, I., & Galhardo, A. (2023). Assessment of psychological (in)flexibility in the Portuguese population: Validation of the short version of the Multidimensional Psychological Flexibility Inventory (MPFI-24). Portuguese Journal of Behavioural and Social Research, 9(1), 1–19. https://doi.org/10.31211/rpics.2023.9.1.285
MPFI - Spanish
MPFI - SpanishReferences:
Simkin, H., Freiberg-Hoffmann, A., Caselli, G., Prozzillo, P., Rogge, R. D., & Wilson, K. G. (2023). Adaptation and Validation into Spanish of the Multidimensional Psychological Flexibility Inventory (MPFI): evidence of internal validity andfactorial Invariance. Revista AJAYU, 21(2), 111–130. https://doi.org/10.35319/ajayu.212188 The MPFI Spanish version is in the Appendix.
MPFI - Swedish
MPFI - SwedishReferences:
Tabrizi, F. F., Larsson, A., Grönvall, H., Söderstrand, L., Hallén, E., Champoux-Larsson, M., Lundgren, T., Sundström, F., Lavefjord, A., Buhrman, M., Sundin, Ö,. McCracken, L., Åhs, F., & Jansson, B. (2023). Psychometric evaluation of the Swedish Multidimensional Psychological Flexibility Inventory (MPFI). Cognitive Behaviour Therapy, 52(4), 295-316. DOI: 10.1080/16506073.2022.2153077
Sundström, F.T.A., Lavefjord, A., Buhrman, M., & McCracken, L.M. (2023). Assessing Psychological Flexibility and Inflexibility in Chronic Pain Using the Multidimensional Psychological Flexibility Inventory (MPFI). The Journal of Pain, 24(5), 770-781. https://doi.org/10.1016/j.jpain.2022.11.010
MPFI - Turkish
MPFI - TurkishGİZEM ULUBAY (2020) ÇOK BOYUTLU PSİKOLOJİK ESNEKLİK ENVANTERİNİN TÜRKÇEYE UYARLANMASI. T.C. BALIKESİR ÜNİVERSİTESİ, Master's Thesis.
MPFI-24 - French Validation
MPFI-24 - French ValidationMultidimensional Psychological Flexibility Inventory short form (MPFI-24) French Validation
Grégoire, S. et al (2020). Validation of the English and French versions of the multidimensional psychological flexibility inventory short form (MPFI-24). Journal of Contextual Behavioral Science, 18, 99-110. https://doi.org/10.1016/j.jcbs.2020.06.004 The French Translation of the MPFI is in Appendix A.
Personalized Psychological Flexibility Index (PPFI)
Personalized Psychological Flexibility Index (PPFI)Kashdan, T. B., Disabato, D. J., Goodman, F. R., Doorley, J. D., & McKnight, P. E. (2020). Understanding psychological flexibility: A multimethod exploration of pursuing valued goals despite the presence of distress. Psychological Assessment, 32(9), 829–850. https://doi.org/10.1037/pas0000834
Cherry, K.M., Vander Hoeven, E., Patterson, T.S., & Lumley, M.N. (2021). Defining and measuring “psychological flexibility”: A narrative scoping review of diverse flexibility and rigidity constructs and perspectives. Clinical Psychology Review, 84, 101973. https://www.sciencedirect.com/science/article/abs/pii/S0272735821000167
The PPFI English version and in Persian version in this Journal of Contextual Behavioral Science article Appendix A.
PPFI - Chinese
PPFI - ChineseReferences:
Fang, S., Huang, M, Wang, Y. (2023). Reliability and validity of the Chinese version of personalized psychological flexibility index (C-PPFI) in college students. Journal of Contextual Behavioral Science, 28, 23-32. DOI: 10.1016/j.jcbs.2023.03.008
Xia, W., Yan, M., Jiang, W., Ou, M., Xie, C., Liu, X., & Xu, X. (2023). Psychometric validation of the modified Chinese version of the personalized psychological flexibility index in patients with cancer. Asia-Pacific Journal of Oncology Nursing, 10(6), 100240. DOI: 10.1016/j.apjon.2023.100240.
PPFI - Persian
PPFI - PersianAkbari, M., Disabato, D., Seydavi, M. & Zamani, E. (2021). The Persian Personalized Psychological Flexibility Index (P-PPFI): Psychometric properties in a general population sample of Iranians. Journal of Contextual Behavioral Science, 22, 32-43. https://doi.org/10.1016/j.jcbs.2021.09.004 The Persian PPFI is in Appendix A.
Psy-Flex
Psy-FlexThe Psyflex is a six-item self-report questionnaire assessing all six processes involved in ACT in a state form with high temporal specificity (last week).
The Psy-Flex measure is available https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
References:
Benoy, C., Knitter, B., Schumann, I., Bader, K., Walter, M., & Gloster, A.T. (2019). Treatment sensitivity: Its importance in the measurement of psychological flexibility. Journal of Contextual Behavioral Science, 13, 121-125. https://doi.org/10.1016/j.jcbs.2019.07.005
Gloster, A.T. et al (2021) Psy-Flex: A contextually sensitive measure of psychological flexibility. Journal of Contextual Behavioral Science, 22, 13-23. https://doi.org/10.1016/j.jcbs.2021.09.001 The Psy-Flex measure is in the Appendix.
Validation of Psy-Flex for Adolescents (PsyFlex-A): Soares, R., Cunha, M., Massano-Cardoso, I., & Galhardo, A. (2023). Assessing psychological flexibility in adolescents: Validation of PsyFlex-A . Portuguese Journal of Behavioral and Social Research, 9(1), 1–18. DOI: 10.31211/rpics.2023.9.1.284
Jo, D., Seong, B., & Yang, E. (2023). Psychometric properties of the Psy-flex scale: A validation study in a community sample in Korea. Journal of Contextual Behavioral Science, 30, 70-79. https://doi.org/10.1016/j.jcbs.2023.09.004
Psy-Flex (Chinese)
Psy-Flex (Chinese)Psy-Flex Chinese version by: C. Y. Y. Chong
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
References:
Fang, S., Ding, D., Huang, M., & Zheng, Q. (2024). Chinese version of the Simplified Psychological Flexibility Scale-6 (C-Psy-Flex): study of its psychometric properties from the perspective of classical test theory and network analysis. Journal of Contextual Behavioral Science. https://doi.org/10.1016/j.jcbs.2024.100769
Psy-Flex (Dutch)
Psy-Flex (Dutch)Psy-Flex Dutch version by: Tom Van Daele
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Finnish)
Psy-Flex (Finnish)Psy-Flex Finnish version by: Raimo Lappalainen
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (French)
Psy-Flex (French)Psy-Flex French version by Jean-Louis Monestès
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (German)
Psy-Flex (German)German Validation Study: Gloster, A.T. et al (2021) Psy-Flex: A contextually sensitive measure of psychological flexibility. Journal of Contextual Behavioral Science, 22, 13-23. https://doi.org/10.1016/j.jcbs.2021.09.001
The Psy-Flex German version is available at https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Greek)
Psy-Flex (Greek)Validation study: Paraskeva-Siamata, M., Spyridou, G., Gloster, A., & Karekla, M., (2018, July). Psyflex: Validation of a new psychological flexibility measure in a Greek-Cypriot sample. Poster presented at the Association of Contextual Behavior Science annual world conference, Montreal, Canada.
The Psy-Flex Greek version is available at https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Hebrew)
Psy-Flex (Hebrew)Psy-Flex Hebrew version by: D. Mouadeb
https://psychologie.unibas.ch/fileadmin/user_upload/psychologie/Abteilungen/Clinical_Psychology_and_Intervention_Science/docs/psy-flex/psy-flex-heb.pdf
Psy-Flex (Hungarian)
Psy-Flex (Hungarian)Psy-Flex Hungarian version by: Dorottya Őri
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Italian)
Psy-Flex (Italian)Psy-Flex Italian version by: Giovambattista Presti
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Korean)
Psy-Flex (Korean)Psy-Flex Korean version by: D. Jo
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
References
Jo, D., Seong, B., & Yang, E. (2023). Psychometric properties of the Psy-flex scale: A validation study in a community sample in Korea. Journal of Contextual Behavioral Science, 30, 70-79. https://doi.org/10.1016/j.jcbs.2023.09.004 The Psy-Flex Korean version is in the Appendix.
Psy-Flex (Latvian)
Psy-Flex (Latvian)Psy-Flex Latvian version by: Jelena Lubenko
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Montenegrin)
Psy-Flex (Montenegrin)Psy-Flex Montenegrin version by: Iva Ivanovic
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Polish)
Psy-Flex (Polish)Psy-Flex Polish version by Bartosz Kleszcz
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Portuguese)
Psy-Flex (Portuguese)Portuguese version by: David Manuel Dias Neto & Ana Nunes da Silva
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
References:
Cunha, M., Temido, A., Moniz, A., & Galhardo, A. (2024). Assessing psychological flexibility and mental health in adults: The Psy-Flex European Portuguese version. Journal of Contextual Behavioral Science, 32, 100730. DOI: 10.1016/j.jcbs.2024.100730
Cunha, M., Temido, A., Pinto-Gouveia, A., & Galhardo, A. (2023). Assessing psychological flexibility by the Psy-Flex and its relationship with mental health. European Psychiatry, 66(S1), S368-S369. DOI: 10.1192/j.eurpsy.2023.800
Cunha, M., & Temido, A. M. (2021). A versão Portuguesa da Psy-Flex [Manuscrito não publicado]. Instituto Superior Miguel Torga, Centro de Investigação em Neuropsicologia e Intervenção Cognitivo-comportamental da Universidade de Coimbra.
Psy-Flex (Romanian)
Psy-Flex (Romanian)Psy-Flex Romanian version by: Adriana Baban
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Slovenian)
Psy-Flex (Slovenian)Psy-Flex Slovenian version by: David Gosar
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Spanish)
Psy-Flex (Spanish)Psy-Flex Spanish version by Francisco Ruiz Jiménez, Maria Belén García-Martín & Miguel A. Segura-Vargas
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Swedish)
Psy-Flex (Swedish)Psy-Flex Swedish version by: David Nilsson
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
Psy-Flex (Turkish)
Psy-Flex (Turkish)Psy-Flex Turkish version by: Gökçen Aydın
https://psychologie.unibas.ch/en/faculty/centers/clinical-psychology-and-intervention-science/research/research-projects/psy-flex/#c24662
References:
Yıldırım, M., Aziz, I.A. (2023). Turkish validation of the Psy-Flex Scale and its association with resilience and social support. Environment and Social Psychology, 8(1), 1513. DOI: 10.18063/esp.v8.i1.1513
Problem Specific Psychological Flexibility or Inflexibility Measures
Problem Specific Psychological Flexibility or Inflexibility MeasuresAAQ variations for specific problems
AAQ variations for specific problemsThe AAQ has been developed for specific disorders, syndromes, and types of chronic disease.
AADQ (Diabetes)
AADQ (Diabetes)Gregg, J.A., Callaghan. G.M., Hayes, S.C., & Glenn-Lawson, J.L. (2007). Improving diabetes self-management through acceptance, mindfulness, and values: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 75(2), 336-343.
AADQ - Chinese
AADQ - ChineseXIE Chanjuan, XU Xianghua, OU Meijun, MAO Ting, CHEN Yongyi (2019) Chineseization and reliability and validity test of Diabetes Acceptance and Action Questionnaire. 护理研究, 1, 37-41. Article retrieved from CAOD.
AADQ - German
AADQ - GermanSchmitt, A., Gahr, A., Hermanns, N., Kulzer, B. & Haak, T. (2013). Evaluation der deutschen Fassung des Fragebogens AADQ zur Diabetesakzeptanz [Evaluation of the AADQ (German Version) in Measuring Diabetes Acceptance]. Diabetes, Stoffwechsel und Herz, 22, 9-15. The German AADQ is on page 10. Retrieved from https://www.researchgate.net/publication/235768284_Evaluation_of_the_AADQ_German_Version_in_Measuring_Diabetes_Acceptance
AADQ - Japanese
AADQ - JapaneseSaito, J., Shoji, W. & Kumano, H. (2018) The reliability and validity for Japanese type 2 diabetes patients of the Japanese version of the acceptance and action diabetes questionnaire. BioPsychoSocial Medicine, 12, 9. https://doi.org/10.1186/s13030-018-0129-9
AADQ - Persian
AADQ - PersianRajaeiramsheh, F., Rezaie, Z., Davoudi, M. et al. (2021) Psychometric properties of the Persian versions of acceptance and action diabetes questionnaire (AADQ) and the diabetes acceptance and action scale (DAAS), in Iranian youth with type 1 diabetes. J Diabetes Metab Disord. https://doi.org/10.1007/s40200-021-00796-1 AADQ Persian Translation is in the article's Supplementary Information.
AADQ - Turkish
AADQ - TurkishKaradere, M. E., Yavuz, K. F., Asafov, E. Y., & Küçükler, F. K. (2019). Reliability and Validity of a Turkish Version of the Acceptance and Action Diabetes Questionnaire. Psychiatry investigation, 16(6), 418–424. https://doi.org/10.30773/pi.2019.02.26.2 The Turkish AADQ is in the Supplementary Material.
AAEpQ (Epilepsy)
AAEpQ (Epilepsy)Lundgren, T., Dahl, J., Melin, L., & Kies, B. (2006). Evaluation of acceptance and commitment therapy for drug refractory epilepsy: a randomized controlled trial in South Africa—a pilot study. Epilepsia, 47(12), 2173-2179.
Lundgren, L., Dahl, J., & Hayes, S.C. (2008). Evaluation of mediators of change in the treatment of epilepsy with acceptance and commitment therapy. Journal of Behavioral Medicine, 31(3), 225,235.
AAQ for Cancer
AAQ for CancerAAQ for use with cancer patients.
Arch, J.J. & Mitchell, J. L. (2016). An acceptance and commitment therapy (ACT) group intervention for cancer survivors experiencing anxiety at re-entry. Psycho-Oncology, 25(5), 610-615.
AAQ-ABI (acquired brain injury)
AAQ-ABI (acquired brain injury)The AAQ-ABI is a 9 item scale assessing both acceptance and avoidance of thoughts that may arise as a result of brain injury. It uses a 5-point Likert scale (0=’not at all true’ to 4=’very true’) with scores ranging from 0 to 36. Higher scores indicate greater psychological inflexibility. The AAQ-ABI correlates highly with the Acceptance and Action Questionnaire-II (AAQ-II) (rs= .70, N= 75, p< .01) (Whiting et al., in press).
Citations:
Faulkner, J.W., Snell, D.L., Theadom, A., Mahon, S., Barker-Collo, S. & Skirrow, P. (2021) Psychological flexibility in mild traumatic brain injury: an evaluation of measures. Brain Injury, 35(9), 1103-1111, DOI: 10.1080/02699052.2021.1959062
Whiting, D. L., Deane, F. P., Ciarrochi, J., McLeod, H. J., & Simpson, G. K. (2015). Validating measures of psychological flexibility in a population with acquired brain injury. Psychological Assessment, 27(2), 415–423. https://doi.org/10.1037/pas0000050
AAQ-ABI - Dutch
AAQ-ABI - DutchRauwenhoff, J., Peeters, F., Bol, Y., & Van Heugten, C. (2021). Measuring psychological flexibility and cognitive defusion in individuals with acquired brain injury. Brain Injury, 35(10), 1301-1307. DOI: 10.1080/02699052.2021.1972155
AAQ-AHL (Hearing Loss)
AAQ-AHL (Hearing Loss)Ong, C.W., Whicker, J.J., Muñoz, K., & Twohig, M.P. (2019). Measuring psychological inflexibility in adult and child hearing loss. International Journal of Audiology, 58(10), 643-650. DOI: 10.1080/14992027.2019.1630759
Yang, Y., Liu, Y., Xiao, Y., Zhang, L., Li, Y., Zhu, H., & Bian, J. (2022). Cross-cultural adaptation, reliability, and validity of the Chinese version of the Acceptance and Action Questionnaire-Adult Hearing Loss. International Journal of Audiology, 61 (10), 876-881. DOI: 10.1080/14992027.2021.2002954
San Miguel, G.G., Muñoz, K., Barrett,T.S. & Twohig, M.P. (in press) Acceptance and Action Questionnaire-Adult Hearing Loss (AAQ-AHL): validation with hearing aid users. International Journal of Audiology. DOI: 10.1080/14992027.2022.2142161
AAQ-AHL - Chinese
AAQ-AHL - ChineseYang, Y., Liu, Y., Xiao, Y., Zhang, L., Li, Y., Zhu, H., & Bian, J. (2021 in press) Cross-cultural adaptation, reliability, and validity of the Chinese version of the Acceptance and Action Questionnaire-Adult Hearing Loss. International Journal of Audiology. DOI: 10.1080/14992027.2021.2002954
AAQ-D (Depression)
AAQ-D (Depression)Cooper, E. A. (2009) Acceptance and commitment therapy and depression: the development of a depression specific process measure. DPsyc (Clin) dissertation, University of
Wollongong. http://ro.uow.edu.au/theses/795 The AAQ-D is in the appendix.
AAQ-Ex (Exercise)
AAQ-Ex (Exercise)Staats, S. B., & Zettle, R. D. (2011, November). The Acceptance and Action Questionnaire for Exercise (AAQ-Ex). Poster session presented at the meeting of the Association for Behavioral and Cognitive Therapies, Toronto.
Staats, S. B., & Zettle, R. D. (2012, July). Exercise behavior and the Acceptance and Action Questionnaire for Exercise (AAQ-Ex). Poster session presented at the meeting of the Association for Contextual Behavioral Science, Washington, DC.
Staats, S. B. (2014). Development and Validation of the Acceptance and Action Questionnaire for Exercise(Unpublished master's thesis). Wichita State University, Wichita, Kansas.
Staats, S. B. (2014, June). Development and validation of the Acceptance and Action Questionnaire for Exercise. In R. D. Zettle, Relevance of ACT processes in promoting health behaviors: Assessment and intervention: Contextual Medicine SIG sponsored. Symposium conducted at the world conference of the Association for Contextual Behavioral Science, Minneapolis, Minnesota.
***NOTE*** THE 15-ITEM VERSION IS PREFERRED. Please use this one if possible. See attached thesis for normative information on both 15- and 11-item versions (Table 26; p. 89). Thanks! :D
AAQ-Ex - Brazilian Portuguese version
AAQ-Ex - Brazilian Portuguese versionAAQ-EX Brazilian translation and adaptation: Lucena-Santos, Oliveira, & Pinto-Gouveia, 2014 This is translation has not been validated.
Corresponding author: Paola Lucena-Santos.
E-mail: paolabc2.lucena@gmail.com
WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
AAQ-II-P (Pain)
AAQ-II-P (Pain)Reneman MF, Kleen M, Trompetter HR, Schiphorst Preuper HR, Köke A, van Baalen B, Schreurs KM. (2014) Measuring avoidance of pain: validation of the Acceptance and Action Questionnaire II-pain version. Int J Rehabil Res, 37(2), 125-129. doi: 10.1097/MRR.0000000000000044
AAQ-II-P - Dutch
AAQ-II-P - DutchReneman, M. et al (2014). Measuring avoidance of pain validation of the Acceptance and Action Questionnaire II-pain version. International Journal of Rehabilitation Research, 37(2), 125-129. http://doi.org/10.1097/MRR.0000000000000044
AAQ-II-P - German
AAQ-II-P - GermanMajeed R, Faust I, Hüppe M, & Hermann C. (2021 in press). Messung von schmerzbezogener Erlebensvermeidung: Analyse des Acceptance and Action Questionnaire-II-Pain bei Patienten mit chronischem Schmerz [Measurement of pain-related experiential avoidance: analysis of the Acceptance and Action Questionnaire-II-Pain in patients with chronic pain]. Schmerz, 35, 401–411. https://doi.org/10.1007/s00482-021-00537-6 The German Version of the AAQ-II-P is in Table 3.
AAQ-OC (Obsessions and Compulsions)
AAQ-OC (Obsessions and Compulsions)The AAQ for Obsessions and Compulsions (AAQ-OC) is a 13-item self-report measure of experiential avoidance in response to unwanted intrusive thoughts.
The original paper describing its psychometric properties is published here:
Jacoby, R. J., Abramowitz, J. A., Buchholz, J. L., Reuman, L., & Blakey S. M. (2018). Experiential avoidance in the context of obsessions: Development and validation of the Acceptance and Action Questionnaire for Obsessions and Compulsions. Journal of Obsessive Compulsive and Related Disorders, 19, 34-43. doi: 10.1016/j.jocrd.2018.07.003.
Abstract: The unwillingness to remain in contact with obsessions and anxiety (i.e., experiential avoidance, EA) may explain how normally occurring unwanted intrusive thoughts develop into clinical obsessions as seen in obsessive compulsive disorder (OCD). Studies examining the relationship between EA and OC symptoms are mixed, potentially because the existing self-report measure of EA (i.e., the Acceptance and Action Questionnaire, AAQ-II) is a general measure that does not adequately capture EA specific to obsessions and compulsions. Thus, we aimed to develop and evaluate an OC-specific version of the AAQ-II. First, we used exploratory factor analysis to empirically reduce an initial pool of 49 items (adapted from original AAQ-II items to reference “intrusive thoughts”) to 13 items. A two-factor solution (Valued Action and Willingness) provided the best fit to the data, accounting for 60.57% of the variance. Second, the reduced AAQ-OC was administered, along with other self-report measures, to an independent sample of adults. The AAQ-OC subscales evidenced good internal consistency as well as convergent, discriminant, and incremental validity. Future work examining the psychometric properties of the AAQ-OC in a clinical sample, as well as the measure's treatment sensitivity are needed.
The AAQ-OC is linked below in PDF format and is downloadable for members. All 13-items are summed to yield a total score of experiential avoidance in response to unwanted intrusive thoughts. There are also two subscales representing impairments in: Valued Action (sum of items 1, 3, 4, 6, 8, 9, 10, and 12) and Willingness (sum of items 2, 5, 7, 11, and 13).
Contact Dr. Ryan Jane Jacoby with questions or comments: rjjacoby@mgh.harvard.edu
References:
Barrett, K., O’Connor, M. & McHugh, L. A. (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
Jacoby, R. J., Abramowitz, J. A., Buchholz, J. L., Reuman, L., & Blakey S. M. (2018). Experiential avoidance in the context of obsessions: Development and validation of the Acceptance and Action Questionnaire for Obsessions and Compulsions. Journal of Obsessive Compulsive and Related Disorders, 19, 34-43. doi: 10.1016/j.jocrd.2018.07.003.
AAQ-OC - Persian
AAQ-OC - PersianEsmail Soltani, et al. (2020) Psychometric properties of the Persian version of the acceptance and Action Questionnaire for obsessions and compulsions (AAQ-OC). Journal of Obsessive-Compulsive and Related Disorders, 27, 100582. https://doi.org/10.1016/j.jocrd.2020.100582
AAQ-S (Stigma)
AAQ-S (Stigma)The AAQ-S is a 21 item measure of psychological flexibility/inflexibility with stigmatizing thoughts. The measure includes two subscales (psychological flexibility and psychological inflexibility), which can be analyzed separately or combined into a total score.
The AAQ-S can be downloaded from the Utah State University ACT Research Group.
The citation for the measurement development/validation paper is:
Trigueros, R., Navarro-Gómez, N., Aguilar-Parra, J. M., & Cangas, A. J. (2020). Factorial Structure and Measurement Invariance of the Acceptance and Action Questionnaire-Stigma (AAQ-S) in Spain. International Journal of Environmental Research and Public Health, 17(2), 658. https://doi.org/10.3390/ijerph17020658
Levin, M.E., Luoma, J.B., Lillis, J., Hayes, S.C. & Vilardaga, R. (2014). Developing a measure of psychological flexibility with stigmatizing thoughts. Journal of Contextual Behavioral Science, 3, 21-26.
AAQ-S - Korean
AAQ-S - KoreanLee, H., Kwon, M., & Seo, K. (2021). Validity and Reliability of the Korean Version of the Acceptance and Action Questionnaire-Stigma (AAQ-S-K). Healthcare, 9(10),1355. https://doi.org/10.3390/healthcare9101355
AAQ-S - Spanish
AAQ-S - SpanishValdivia-Salas, S., Martín-Albo, J., Cruz, A., Villanueva-Blasco, V.J., & Jiménez T.I. (2021) Psychological Flexibility With Prejudices Increases Empathy and Decreases Distress Among Adolescents: A Spanish Validation of the Acceptance and Action Questionnaire–Stigma. Frontiers in Psychology, 11, 3911. https://doi.org/10.3389/fpsyg.2020.565638
Trigueros, R., Navarro-Gómez, N., Aguilar-Parra, J. M., & Cangas, A. J. (2020). Factorial Structure and Measurement Invariance of the Acceptance and Action Questionnaire-Stigma (AAQ-S) in Spain. International Journal of Environmental Research and Public Health, 17(2), 658. http://dx.doi.org/10.3390/ijerph17020658 The AAQ-S Spanish translation is in Appendix A.
AAQ-SA (Substance abuse)
AAQ-SA (Substance abuse)The AAQ for Substance Abuse (AAQ-SA) is a measure of psychological flexibility in relation to substance misuse.
The original paper describing it pscychometric properties is:
Luoma, J. B., Drake, C., Hayes, S. C., Kohlenberg, B. (2011). Substance Abuse and Psychological Flexibility: The Development of a New Measure. Addiction Research and Theory, 19(1), 3-13.
The paper can be downloaded here: http://contextualscience.org/node/5681
Below is the abstract of that study
Psychological flexibility is a relatively new clinical construct targeted by Acceptance and Commitment Therapy, a behavior analytic treatment incorporating mindfulness and values interventions, among other processes. Poor psychological flexibility has been shown to relate to clinical problems as well as normative life challenges, and efforts to increase psychological flexibility have correlated with improvements for a variety of psychological difficulties, including substance abuse. The Acceptance and Action Questionnaire (AAQ) is currently the standard measure of psychological flexibility, but in substance misusing samples, has not shown adequate psychometric properties. Content-specific variants of the AAQ have been effective in other treatment domains, suggesting that a substance abuse focused version of the AAQ may be useful. This paper details the construction and initial validation of such a measure, the AAQ-SA, which demonstrated good internal consistency, factor structure, and construct validity. In addition, the AAQ-SA appeared to be empirically distinguishable from the AAQ. Future researchers are advised to address limitations of the current work and encouraged to expand the empirical database on substance abuse treatment with this new measure.
The measure is attached to this webpage along with scoring instructions.
AAQ-SA - Arabic
AAQ-SA - ArabicElkalla, Ibrahem & El-Gilany, Abdel-Hady & Elwasify, Mohamed. (2020). Acceptance and action questionnaire − substance abuse: translation into arabic, content validity and reliability. Egyptian Journal of Psychiatry, 41(2), 82-88.
Full Text available on the journal website.
AAQ-SA - French
AAQ-SA - FrenchIl s'agit d'une traduction libre du AAQ-SA et qui a été révisée par des membres francophones de la communauté ACBS. Pour usage clinique seulement car elle n'a pas été validée empiriquement. Utile auprès d'une population au prise avec des problématiques reliées à la consommation de drogues et/ou d'alcool.
AAQ-SA - Portuguese
AAQ-SA - PortugueseSequeira, F. & Galhardo, A. (2018) Questionário de Aceitação e Ação para Abuso de Substâncias: desenvolvimento da versão portuguesa, estudo exploratório da estrutura fatorial e propriedades psicométricas. ISMT, Dissertation. The Portuguese AAQ-SA is in the Appendix.
AAQ-SA - Spanish
AAQ-SA - SpanishHilda A. Sánchez-Millán, Alfredo Alicea-Cruz, Coralee Pérez Pedrogo (2021 in press) Measuring psychological flexibility: The cultural adaptation and psychometric properties of the AAQ for substance abuse among Spanish speaking population in correctional and community settings. Journal of Contextual Behavioral Science. https://doi.org/10.1016/j.jcbs.2021.11.002 The Spanish version of the AAQ-SA items are in Appendix A.
Luis Ángel Pérez-Romero, Ariel Vite-Sierra (2020) Midiendo la flexibilidad psicológica: validación del Cuestionario de Aceptación y Acción en el abuso de drogas [Measuring the psychological flexibility: Validationof Acceptance and Action Questionnaire on substance abuse]. Psicología y Salud, 30(1), 95-104. https://doi.org/10.25009/pys.v30i1.2621
AAQ-SA - Turkish
AAQ-SA - TurkishUygur H, Yavuz KF, Eren I, Uygur OF, Selcuk M, Varsak N, Ozbek Yildirim S, Demirel B. (2020) Reliability and Validity of the Turkish Version of the Acceptance and Action Questionnaire-Substance Abuse (AAQ-SA) on a Clinical Sample. Psychiatry and Clinical Psychopharmacology, 30(1), 47-54. DOI: 10.5455/PCP.20200320085704
AAQ-SA - Urdu
AAQ-SA - UrduAn AAQ for Substance Abuse (AAQ-SA) was created in French by Habiba Ilyas and attached to this page. See the file for contact info.
AAQ-SI (suicidal Ideation)
AAQ-SI (suicidal Ideation)Boffa, J.W., Tock, J.L., Morabito, D.M. et al. Measuring Psychological Inflexibility of Suicidal Thoughts: The Acceptance and Action Questionnaire for Suicidal Ideation (AAQ-SI). Cogn Ther Res (2022). https://doi.org/10.1007/s10608-022-10309-w
AAQ-Sports
AAQ-SportsBisagni, D., Bisagni, M., & Vaccaro, M. (2018). Mindfulness e flessibilità psicologica nella pratica sportiva: validazione della versione italiana della State Mindfulness Scale for Physical Activity (SMS-PA) e della versione per lo sport dell’Acceptance and Action Questionnaire (AAQ-II) [Mindfulness and psychological flexibility in sport practice: Validation of the italian version of the SMS-PA and the sports version of the AAQ-II]. Psicoterapia cognitiva e comportamentale, 24(2), 153-173.
AAQ-Sports - Italian
AAQ-Sports - ItalianBisagni, D., Bisagni, M., & Vaccaro, M. (2018). Mindfulness e flessibilità psicologica nella pratica sportiva: validazione della versione italiana della State Mindfulness Scale for Physical Activity (SMS-PA) e della versione per lo sport dell’Acceptance and Action Questionnaire (AAQ-II) [Mindfulness and psychological flexibility in sport practice: Validation of the italian version of the SMS-PA and the sports version of the AAQ-II]. Psicoterapia cognitiva e comportamentale, 24(2), 153-173.
AAQ-TS (Trauma Specific)
AAQ-TS (Trauma Specific)Pinto-Gouveia, J., Carvalho, T., Cunha, M., Duarte, J., Walser, R.D. (2015). Psychometric properties of the Portuguese version of the Acceptance and Action Questionnaire-Trauma Specific (AAQ-TS): A study with Portuguese Colonial War Veterans. J Affect Disord., 185, 81-89. DOI: 10.1016/j.jad.2015.06.023
AAQ-TS - Portuguese version
AAQ-TS - Portuguese versionPinto-Gouveia, J., Carvalho, T., Cunha, M., Duarte, J., Walser, R.D. (2015). Psychometric properties of the Portuguese version of the Acceptance and Action Questionnaire-Trauma Specific (AAQ-TS): A study with Portuguese Colonial War Veterans. J Affect Disord., 185, 81-89.
DOI: 10.1016/j.jad.2015.06.023
AAQ-TTM (Trichotillomania)
AAQ-TTM (Trichotillomania)Houghton DC, Compton SN, Twohig MP, et al. (2014). Measuring the role of psychological inflexibility in Trichotillomania. Psychiatry Research, 220(1-2):356-361. http://doi.org/10.1016/j.psychres.2014.08.003.
AAQ-US (University Students)
AAQ-US (University Students)Levin, M.E., Krafft, J., Pistorello, J., & Seeley, J.R. (2019) Assessing psychological inflexibility in university students: Development and validation of the acceptance and action questionnaire for university students (AAQ-US). Journal of Contextual Behavioral Science, 12, 199-206. https://doi.org/10.1016/j.jcbs.2018.03.004 The AAQ-US can be downloaded from the Utah State University ACT Research Group.
AAQ-US - Portuguese
AAQ-US - PortugueseGalhardo, A., Neto, M., Monteiro, B. et al. (2022 in press). Psychological inflexibility in university students: the european portuguese version of the acceptance and action questionnaire—university students. Current Psychology. https://doi.org/10.1007/s12144-022-04174-9
Machado, A.B.C., Zancan, R.K., & Oliveira, M.S. (2021). Adaptação do Acceptance and Action Questionnaire for University Students (AAQ-US) para o Português Brasileiro [Adaptation of the Acceptance and Action Questionnaire for University Students (AAQ-US) for Brazilian Portuguese]. Contextos Clínicos, 14 (3). https://doi.org/10.4013/ctc.2021.143.13 The Portuguese translation of the AAQ-US items are in Tabela 1.
Neto, M.J.O. & Galhardo, A. (2020) Estudo da estrutura fatorial e propriedades psicométricas da versão portuguesa do Acceptance and Action Questionnaire – University Students (AAQ-US). ISMT, Dissertation. https://dspace.ismt.pt/handle/123456789/1211
AAQ-US - Spanish
AAQ-US - SpanishBarbosa Güiza, A. (2020.). Propiedades psicométricas del cuestionario aceptación y compromiso en estudiantes universitarios (AAQ-US) en el contexto colombiano. Escuela de Posgrados. Konrad Lorenz, Thesis.
AAQ-US - Turkish
AAQ-US - TurkishKuru, T., Karadere, M.E., Burhanm H.S., & Safak, Y. (2021) Reliability and Validity Study of the Turkish Version of the Acceptance and Action Questionnaire for University Students. Psychiatry and Behavioral Sciences, 11(1), 18-24. http://doi.org/10.5455/PBS.20201202024935
AAQ-W (weight)
AAQ-W (weight)Acceptance and Action Questionnaire for Weight-Related Difficulties. The scale and additional information (scoring instructions and a brief summary of psychometric properties) are attached below.
The AAQ-W can also be found on stevenchayes.com
References:
Lillis, J., & Hayes, S.C. (2008). Measuring avoidance and inflexibility in weight related problems. International Journal of Behavioral Consultation and Therapy, 4(4), 348-354.
Weineland, S., Lillis, J., & Dahl, J. (2013). Measuring experiential avoidance in a bariatric surgery population--psychometric properties of AAQ-W. Obesity research & clinical practice, 7(6), e464–e475.
Manwaring, J., Hilbert, A., Walden, K., Bishop, E. R., & Johnson, C. (2018). Validation of the acceptance and action questionnaire for weight-related difficulties in an eating disorder population. Journal of Contextual Behavioral Science, 7, 1-7
References for AAQ-W Revised Versions:
Palmeira, L., Cunha, M., Pinto-Gouveia, J., Carvalho, S., & Lillis, J. (2016) New developments in the assessment of weight-related experiential avoidance (AAQW-Revised). Journal of Contextual Behavioral Science, 5(3), 193-200. https://doi.org/10.1016/j.jcbs.2016.06.001
Dochat, C., Afari, N., Wooldridge, J.S., Herbert, M.S., Gasperi, M., & Lillis, J. (2020) Confirmatory factor analysis of the Acceptance and Action Questionnaire for Weight-Related Difficulties-Revised (AAQW-R) in a United States sample of adults with overweight and obesity. Journal of Contextual Behavioral Science, 15, 189-196. https://doi.org/10.1016/j.jcbs.2020.01.006
AAQ-W - Brazilian Portuguese version
AAQ-W - Brazilian Portuguese versionAAQ - W Tradução e adaptação brasileira: Lucena-Santos, Pinto-Gouveia, & Oliveira, 2014. This translation has not been validated.
Corresponding author: Paola Lucena-Santos.
E-mail: paolabc2.lucena@gmail.com
WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra
AAQ-W - Persian
AAQ-W - PersianPirmoradi, M.R., Asgharzadeh, A., Birashk, B. et al. (2021) Psychometric properties of the Persian version of the weight-related experiential avoidance (AAQW): overweight and obese treatment seeker at the clinical setting. BMC Psychiatry, 21, 335. https://doi.org/10.1186/s12888-021-03352-6
AAQ-W - Spanish
AAQ-W - SpanishIturbe, I., Echeburúa, E., & Maiz, E. (2023 in press). Psychometric properties of the Spanish Acceptance and Action Questionnaire for Weight-Related Difficulties-Revised (AAQW-R). Psychological assessment, 35(5), e12–e21. https://doi.org/10.1037/pas0001224
AAQ-W - Swedish
AAQ-W - SwedishWeineland, S., Lillis, J., & Dahl, J. (2013). Measuring experiential avoidance in a bariatric surgery population--psychometric properties of AAQ-W. Obesity research & clinical practice, 7(6), e464–e475.
AAQW-R Turkish
AAQW-R TurkishTurksih form of AAQW-R based on Palmeira's revised version of AAQ weight.
Burhan H. S. , Kuru, T. & (2023) RELIABILITY AND VALIDITY STUDY OF THE TURKISH VERSION OF THE ACCEPTANCE AND ACTION QUESTIONNAIRE FOR WEIGHT-REVISED. Journal of Cognitive-Behavioral Psychotherapy and Research, 12 (1), 65-70. doi:10.5455/JCBPR.127897
AAQH (Hoarding)
AAQH (Hoarding)Krafft, J., Ong, C.W., Twohig, M.P., Levin, M.E. (2019) Assessing psychological inflexibility in hoarding: The Acceptance and Action Questionnaire for Hoarding (AAQH). Journal of Contextual Behavioral Science, 12, 234-242. https://doi.org/10.1016/j.jcbs.2018.08.003 The AAQH is in the Appendix. The AAQH can be downloaded from the Utah State University ACT Research Group.
Ong, C.W., Krafft, J., Levin, M.E., & Michael P. Twohig, M.P. (2021). A systematic review and psychometric evaluation of self-report measures for hoarding disorder. Journal of Affective Disorders, 290, 136-148. https://doi.org/10.1016/j.jad.2021.04.082
AIS (Smoking)
AIS (Smoking)The Avoidance and Inflexibility Scale (AIS) assesses ACT processes in the context of cigarette smoking. Reference: Gifford, E. V., Antonuccio, D.O, Kohlenberg, B.S., Hayes, S.C., & Piasecki, M.M. (2002). Combining Bupropion SR with acceptance and commitment-based behavioral therapy for smoking cessation: Preliminary results from a randomized controlled trial. Paper presented at the annual meeting of the Association for Advancement of Behavioral Therapy, Reno, NV.
Gifford, E.V., Kohlenberg, B.S., Hayes, S.C., Antonuccio, D.O., Piasecki, M.M., Rasmussen-Hall, M.L., & Palm, K.M. (2004). Acceptance-based treatment for smoking cessation. Behavior Therapy, 35(4):689–705.
Farris, S.G., Zvolensky, M.J., DiBello, A.M., & Schmidt, N.B. (2015). Validation of the Avoidance and Inflexibility Scale (AIS) among treatment-seeking smokers. Psychological Assessment, 27(2), 467-477. http://doi.org/10.1037/pas0000059
AIS - Greek
AIS - GreekSavvides, S. N. (2014). Evaluating an acceptance and commitment therapy internet-based intervention for smoking cessation in young adults. Dissertation, University of Cyprus. Retrived from https://gnosis.library.ucy.ac.cy/handle/7/39519 The Greek AIS is in the Appendix.
BI-AAQ (Body Image)
BI-AAQ (Body Image)Sandoz, E. K., Wilson, K. G., Merwin, R. M., & Kellum, K. (2013). Assessment of body image flexibility: The Body Image – Acceptance and Action Questionnaire. Journal of Contextual Behavioral Science, 2(1–2), 39-48. http://dx.doi.org/10.1016/j.jcbs.2013.03.002
Acceptance and mindfulness components are increasingly incorporated into treatment for eating disorders with promising results. The development of measures of proposed change processes would facilitate ongoing scientific progress. The current series of studies evaluated one such instrument, the Body Image – Acceptance and Action Questionnaire (BI-AAQ), which was designed to measure body image flexibility. Study one focused on the generation and reduction of items for the BI-AAQ and a demonstration of construct validity. Body image flexibility was associated with increased psychological flexibility, decreased body image dissatisfaction, and less disordered eating. Study two demonstrated adequate internal consistency and test-retest reliability of BI-AAQ. Study three extended findings related to structural and construct validity, and demonstrated an indirect effect of body image dissatisfaction on disordered eating via body image flexibility. Research and clinical utility of the BI-AAQ are discussed. The BI-AAQ is proposed as a measure of body image flexibility, a potential change process in acceptance-oriented treatments of eating disorders.
The BI-AAQ is attached below in .pdf format below and is downloadable for members. All items are summed to yield a score for body image inflexibility or reverse-scored to yield a score for body image flexibility.
Also attached below is a modified version of the BI-AAQ that does not refer specifically to weight and shape.
Contact Emily Sandoz with questions or comments: emilysandoz@louisiana.edu
References:
Sandoz, E. K., Wilson, K. G., Merwin, R. M., & Kellum, K. (2013). Assessment of body image flexibility: The Body Image – Acceptance and Action Questionnaire. Journal of Contextual Behavioral Science, 2(1–2), 39-48. http://dx.doi.org/10.1016/j.jcbs.2013.03.002
Lee, E.B., Smith, B.M., Twohig, M.P., Lensegrav-Benson, T., & Quakenbush-Roberts, B. (2017). Assessment of the body Image-Acceptance and Action Questionnaire in a female residential eating disorder treatment facility. Journal of Contextual Behavioral Science, 6(1), 21-28. https://doi.org/10.1016/j.jcbs.2016.11.004
Soulliard, Z.A. & Vander Wal, J. (2022). Measurement invariance and psychometric properties of three positive body image measures among cisgender sexual minority and heterosexual women. Body Image, 40, 146-157. https://doi.org/10.1016/j.bodyim.2021.12.002
BI-AAQ-5 Short Form
References:
Basarkod, G. Sahdra, B., & Ciarrochi, J. (2018). Body Image–Acceptance and Action Questionnaire–5: An Abbreviation Using Genetic Algorithms. Behavior Therapy, 49(3), 388-402. https://doi.org/10.1016/j.beth.2017.09.006
Soulliard, Z.A. & Vander Wal, J.S. (2022). Measurement invariance and psychometric properties of three positive body image measures among cisgender sexual minority and heterosexual women. Body Image, 40, 146-157. https://doi.org/10.1016/j.bodyim.2021.12.002
BI-AAQ - Arabic
BI-AAQ - ArabicAdel, S. (2019). فعالية برنامج عالجي بالتقبل وااللتزام لتحسين صورة الجسم لدى عينة من ذوات اضطراب الشره العصبى [Efficacy of ACT program to improve body image for Female Bulimia nervosa disorder]. Thesis: University of Alexandria. The Arabic BI-AAQ is in the appendix.
BI-AAQ - Chinese
BI-AAQ - ChineseHe, J., Cai, Z., Chen, X., Lu, T., & Fan, X. (2021). Validation of the Chinese Version of the Body Image Acceptance and Action Questionnaire and the Mediating Role of Body Image Flexibility in the Relationship Between Body Dissatisfaction and Psychological Distress. Behavior Therapy, 52(3), 2021, 539-551. https://doi.org/10.1016/j.beth.2020.07.003
BI-AAQ - Greek
BI-AAQ - GreekKarekla, M., Mavrakia, E.Z., Nikolaoua, P., & Koushioua, M. (2019). Validation of the Greek Version of the Body Image-Acceptance and Action Questionnaire. The European Journal of Counselling Psychology, 8(1). https://doi.org/10.5964/ejcop.v8i1.173 The BI-AAQ Greek Translation is in the Appendix.
BI-AAQ - Persian
BI-AAQ - PersianGivehki, R. et al. (2020) Psychometric Properties of the Body Image Acceptance and Action Questionnaire in Patients with Somatic Symptom and Related Disorders in Kashan City. Iranian Journal of Psychiatry and Behavioral Sciences, 14 (2), e69889. http://doi.org/10.5812/ijpbs.69889
Izaadi, A., Karimi, J., & Rahmani, M. (2013) Psychometric Analysis of Persian Version of Body Image flexibility Questionnaire (BI-AAQ) among University students. Hayat, 19 (3), 56-69.
BI-AAQ - Portuguese
BI-AAQ - PortugueseReferences:
Lucena-Santos, P., Carvalho, S.A., da Silva Oliveira, M., & Pinto-Gouveia, J. (2017). Body-Image Acceptance and Action Questionnaire: su nociva influencia en la ingesta compulsiva y validación psicométrica. [Body-Image Acceptance and Action Questionnaire: Its deleterious influence on binge eating and psychometric validation.] International Journal of Clinical and Health Psychology, 17, 151-160. https://doi.org/10.1016/j.ijchp.2017.03.001 The article is open access.
Ferreira, C., Pinto-Gouveia, J., & Duarte, C. (2011) The Validation of the Body Image Acceptance and Action Questionnaire: Exploring the Moderator Effect of Acceptance on Disordered Eating. InternatIonal Journal of Psychology and Psychological Therapy, 11(3), 327-345.
BI-AAQ - Spanish
BI-AAQ - SpanishHernández-López, M., Cepeda-Benito, A., Geist, T., Torres-Dotor, P., Pomichter, E., & Rodríguez-Valverde, M. (2024). Validation of the Spanish version of the body image acceptance and action questionnaire (BI-AAQ-Spanish): Measurement invariance across cultures. Journal of Contextual Behavioral Science, 32, 100755. https://doi.org/10.1016/j.jcbs.2024.100755 The BI-AAQ-Spanish and BI-AAQ-5 are in the Appendix.
CIAQ (Chronic Illness)
CIAQ (Chronic Illness)Beacham, A.O., Linfield, K., Kinman, C.R., Payne-Murphy, J. (2015). The chronic illness acceptance questionnaire: Confirmatory factor analysis and prediction of perceived disability in an online chronic illness support group sample. Journal of Contextual Behavioral Science, 4 (2), 96-102. https://doi.org/10.1016/j.jcbs.2015.03.001
CVD-AAQ (Cardiovascular Disease)
CVD-AAQ (Cardiovascular Disease)Spatola, C.A., Cappella, E.A., Goodwin, C.L., Baruffi, M., Malfatto, G., Facchini, M., et al. (2014) Development and initial validation of the Cardiovascular Disease Acceptance and Action Questionnaire (CVD-AAQ) in an Italian sample of cardiac patients. Front
Psychol, 5, 1284. https://doi.org/10.3389/fpsyg.2014.01284
CVD-AAQ - Italian
CVD-AAQ - ItalianSpatola, C. A., Cappella, E. A., Goodwin, C. L., Baruffi, M., Malfatto, G., Facchini, M., Castelnuovo, G., Manzoni, G. M., & Molinari, E. (2014). Development and initial validation of the Cardiovascular Disease Acceptance and Action Questionnaire (CVD-AAQ) in an Italian sample of cardiac patients. Frontiers in psychology, 5, 1284. https://doi.org/10.3389/fpsyg.2014.01284
DAAS-R (Diabetes)
DAAS-R (Diabetes)This page hosts the adaptation that David Gillanders and Estelle Barker made of the Diabetes Acceptance and Action Questionnre: The DAAS-R. The measure is freely available to members of ACBS for clinical and research purposes (non commercial), with appropriate acknowledgements and citations of the work. The article describing the DAAS-R is available online at JCBS. The citation is:
Gillanders, D. T. & Barker, E. (2019). Development and initial validation of a short form of the Diabetes Acceptance and Action Scale: The DAAS-Revised (DAAS-R). Journal of Contextual Behavioral Science, 14, 20-28. https://doi.org/10.1016/j.jcbs.2019.08.005
Attached is the author's copy of the manuscript and the final questionnaire.
DAAS - Persian
DAAS - PersianRajaeiramsheh, F., Rezaie, Z., Davoudi, M. et al. (2021) Psychometric properties of the Persian versions of acceptance and action diabetes questionnaire (AADQ) and the diabetes acceptance and action scale (DAAS), in Iranian youth with type 1 diabetes. J Diabetes Metab Disord. https://doi.org/10.1007/s40200-021-00796-1 DAAS Persian Translation is in the article's Supplementary Information.
EACQ (Caregiving)
EACQ (Caregiving)Losada, A., Márquez-González, M., Romero-Moreno, R., & López, J. (2014). Development and validation of the Experiential Avoidance in Caregiving Questionnaire (EACQ). Aging & mental health, 18(7), 897–904. https://doi.org/10.1080/13607863.2014.896868
EACQ - French
EACQ - FrenchClotilde Larochette. (2020) Accompagner les proches-aidants confrontés à la maladie d’Alzheimer ou à un trouble apparenté : vers un programme en ligne centré sur la pleine conscience, la psychologie positive et l’acceptation. Psychologie, Université de Lille.
EACQ - Japanese
EACQ - JapaneseHiroshi Morimoto, Naoko Kishita, Hikaru Kondo, Nélida Tanaka, Yu Abe, & Takashi Muto (2023). Reliability and validity of the Japanese version of the experiential avoidance in caregiving questionnaire (EACQ). Journal of Contextual Behavioral Science, 27, 160-169. DOI: 10.1016/j.jcbs.2023.02.003 The Japanese version of the EACQ is in Appendix A.
EACQ - Spanish
EACQ - SpanishLosada, A., Márquez-González, M., Romero-Moreno, R., & López, J. (2014). Development and validation of the Experiential Avoidance in Caregiving Questionnaire (EACQ). Aging & mental health, 18(7), 897–904. https://doi.org/10.1080/13607863.2014.896868
FAAQ (Food craving)
FAAQ (Food craving)FAAQ
Adrienne Juarascio, Evan Forman, C. Alix Timko, Meghan Butryn, Christina Goodwin (2011). The development and validation of the food craving acceptance and action questionnaire (FAAQ). Eating Behaviors, 12(3), 182-187. https://doi.org/10.1016/j.eatbeh.2011.04.008
Murray, H. B., Zhang, F., Manasse, S. M., Forman, E. M., Butryn, M. L., & Juarascio, A. S. (2022). Validation of the food craving Acceptance and action questionnaire (FAAQ) in a weight loss-seeking sample. Appetite, 168, 105680. https://doi.org/10.1016/j.appet.2021.105680 (Revised 7-item FAAQ.)
Brazilian Portuguese version
Corresponding author: Paola Lucena-Santos. E-mail: paolabc2.lucena@gmail.com WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
FAAQ - Brazilian Portuguese version
FAAQ - Brazilian Portuguese versionBrazilian Portuguese version
Corresponding author: Paola Lucena-Santos. E-mail: paolabc2.lucena@gmail.com WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
FAAQ - Spanish
FAAQ - SpanishManchón, J., Quiles, M., & López-Roig, S. (2021). The Role of Acceptance in Eating Behaviors-Spanish Validation of Food Craving Acceptance and Action Questionnaire (FAAQ-S). Frontiers in psychology, 12, 717886. https://doi.org/10.3389/fpsyg.2021.717886
I-AAQ (Interpersonal Interactions)
I-AAQ (Interpersonal Interactions)AAQ version targetting difficulties in interpersonal interactions
IBSAAQ (Irritable Bowel Syndrome)
IBSAAQ (Irritable Bowel Syndrome)The Irritable Bowel Syndrome Acceptance and Action Questionnaire. The scale and additional information (scoring instructions and a brief summary of psychometric properties) are attached below.
Please contact Nuno Ferreira for further information.
MSAQ (multiple sclerosis)
MSAQ (multiple sclerosis)Pakenham, K.I., & Fleming, M. (2011). Relations between acceptance of multiple sclerosis and positive and negative adjustments. Psychology & Health, 26: 1292-1309. https://doi.org/10.1080/08870446.2010.517838
PAAQ (Parental)
PAAQ (Parental)Cheron DM, Ehrenreich JT, Pincus DB. (2009) Assessment of parental experiential avoidance in a clinical sample of children with anxiety disorders. Child Psychiatry Hum Dev, 40(3):383-403.
Click here for translations of the PAAQ: https://contextualscience.org/parental_acceptance_and_action_questionnaire_paaq
PFSS (Psychological Flexibility in Sport Scale)
PFSS (Psychological Flexibility in Sport Scale)Johles, L., Gustafsson, H., Jansson-Fröjmark, M., Classon, C., Hasselqvist, J. & Lundgren, T. (2020) Psychological Flexibility Among Competitive Athletes: A Psychometric Investigation of a New Scale. Frontiers in Sports and Active Living, 2, 110. https://doi.org/10.3389/fspor.2020.0011 The PFSS was inspired by the AAQ-II and adapted to the sport context to measure the construct of psychological flexibility and the degree to which a person avoids distressing thoughts, emotions, behaviors, or memories. PFSS items are rated on a Likert-type scale ranging from 1 (never true) to 7 (always true).
PFSS - Persian
PFSS - PersianBadinlou, F., Badami, R., Reinebo, G. et al. (2022). The Persian version of the psychological flexibility in sport scale: a psychometric study. BMC Psychology, 10, 250. https://doi.org/10.1186/s40359-022-00962-x
PFSS - Swedish
PFSS - SwedishJohles, L., Gustafsson, H., Jansson-Fröjmark, M., Classon, C., Hasselqvist, J. & Lundgren, T. (2020) Psychological Flexibility Among Competitive Athletes: A Psychometric Investigation of a New Scale. Frontiers in Sports and Active Living, 2, 110. https://doi.org/10.3389/fspor.2020.00110
SA-AAQ (Social Anxiety)
SA-AAQ (Social Anxiety)Social Anxiety specific AAQ
MacKenzie, M. B. & Kocovski, N. L. (2010). Self-reported acceptance of social anxiety symptoms: Development and validation of the Social Anxiety - Acceptance and Action Questionnaire. International Journal of Behavioral Consultation and Therapy, 6, 214 – 232.
The original article and measure/scoring instructions are attached below.
B-SA-AAQ (Brief Social Anxiety - Acceptance and Action Questionnaire)
B-SA-AAQ (Brief Social Anxiety - Acceptance and Action Questionnaire)The SA-AAQ has been evaluated and a shorter version is now available. The Brief Social Anxiety - Acceptance and Action Questionnaire is attached below.
MacKenzie, M. B., Kocovski, N. L., Blackie, R. A., Carrique, L. C., Fleming, J. E., & Antony, M. M. (2017). Development of a brief version of the Social Anxiety – Acceptance and Action Questionnaire. Journal of Psychopathology and Behavioral Assessment, 39, 342-354.
Turkish Version of the Brief Social Anxiety-Acceptance and Action Questionnaire
Turkish Version of the Brief Social Anxiety-Acceptance and Action QuestionnaireReliability and Validity Study of the Turkish Version of the Brief Social Anxiety-Acceptance and Action Questionnaire
Furkan Bahadır Alptekin, Hüseyin Şehit Burhan, Tacettin Kuru
Objective: Experiential avoidance is closely related to social anxiety, which is a condition characterized by intense fear in social situations, including social interactions and performing in front of others.
Material and Methods: The sample of this study consisted of 113 people. The data were obtained using a demographic form, Brief Social Anxiety-Acceptance and Action Questionnaire (B-SA-AAQ), Acceptance and Action Questionnaire-II (AAQ-II), and hospital anxiety and depression scale (HADS). Internal consistency and item-total correlation were evaluated with Cronbach’s alpha coefficient. Confirmatory factor analysis (CFA) was used to test the factor structure. Temporal stability was assessed using the test-retest method.
Results: The Turkish adaptation of the B-SA-AAQ was found to have good internal consistency with a Cronbach’s α coefficient of 0.899. CFA indicated a two-factor structure with acceptable fit indices [χ2: 22.8, degrees of freedom: 13; root mean square error of approximation (RMSEA): 0.0817; RMSEA 90% confidence interval (CI) lower bond: 0.013, RMSEA 90% CI upper bond: 0.136, CFI: 0.978; Tucker-Lewis index: 0.965)]. The B-SA-AAQ and its subscales were significantly correlated with the AAQ-II and HADS (p<0.05). The results of the test-retest correlation analysis indicated temporal stability.
Conclusion: Therefore, the B-SA-AAQ is a reliable and valid scale for measuring experiential avoidance and psychological flexibility in the context of social anxiety.
Keywords: Acceptance and commitment therapy, social phobia, anxiety, depression
Citation: Furkan Bahadır Alptekin, Hüseyin Şehit Burhan, Tacettin Kuru (2023). Reliability and Validity Study of the Turkish Version of the Brief Social Anxiety-Acceptance and Action Questionnaire. Cam and Sakura Med J, 3(1), 6-11.
DOI: 10.4274/csmedj.galenos.2023.2022-12-2
SA-AAQ - Korean
SA-AAQ - KoreanKim Ki-Whan, Kwon Seok-Man (2013) 한국판 사회불안 수용 행동 질문지의 타당화 연구 [Validation of the Korean Version of the Social Anxiety-Acceptance and Action Questionnaire]. 인지행동치료, 13, 3, 489 ~ 510.
SA-AAQ - Persian Version
SA-AAQ - Persian VersionSoltani, E., Bahrainian, S. A., Masjedi Arani, A., Farhoudian, A., & Gachkar, L. (2016). Psychometric Properties of the Persian Version of the Social Anxiety - Acceptance and Action Questionnaire. Iranian journal of psychiatry and behavioral sciences, 10(2), e3753. https://doi.org/10.17795/ijpbs.3753
SA-AAQ - Portuguese
SA-AAQ - PortugueseTomé, F.R. (2014) Como estar entre os outros?: o álcool como uma estratégia de evitamento experiencial na ansiedade social. Universidade de Coimbra, Dissertation. The Portuguese SA-AAQ items are in the dissertation.
SA-AAQ - Thai
SA-AAQ - ThaiSiripanit K., Pisitsungkagarn, K. (2017, March). An Initial Development of the Thai Version of the Social Anxiety – Acceptance and Action Questionnaire (SA-AAQ) for Undergraduate Students. The Asian Conference on Psychology & the Behavioral Sciences 2017. Kobe, Japan. The Thai version of the SA-AAQ is in the appendix.
SPAQ (Sleep)
SPAQ (Sleep)Bothelius, K., Jernelöv, S., Fredrikson, M., McCracken, L. M., & Kaldo, V. (2015). Measuring Acceptance of Sleep Difficulties: The Development of the Sleep Problem Acceptance Questionnaire. Sleep, 38(11), 1815–1822. https://doi.org/10.5665/sleep.5170
TA-AAQ-A (Test Anxiety)
TA-AAQ-A (Test Anxiety)Pires, C. P., Putwain, D. W., Hofmann, S. G., Martins, D. S., MacKenzie, M. B., Kocovski, N. L., & Salvador, M. C. (2020). Assessing psychological flexibility in test situations: The Test Anxiety Acceptance and Action Questionnaire for Adolescents [Monograph Innovaciones en la Evaluación de los Problemas Emocionales en Niños y Adolescentes]. Journal of Psychopathology and Clinical Psychology/Revista de Psicopatología y Psicología Clínica, 25(3), 147-159. https://doi.org/10.5944/rppc.29014
TA-AAQ-A - Portuguese
TA-AAQ-A - PortuguesePires, C. P., Putwain, D. W., Hofmann, S. G., Martins, D. S., MacKenzie, M. B., Kocovski, N. L., & Salvador, M. C. (2020). Assessing psychological flexibility in test situations: The Test Anxiety Acceptance and Action Questionnaire for Adolescents [Monograph Innovaciones en la Evaluación de los Problemas Emocionales en Niños y Adolescentes]. Journal of Psychopathology and Clinical Psychology/Revista de Psicopatología y Psicología Clínica, 25(3), 147-159. https://doi.org/10.5944/rppc.29014
TAAQ (Teachers)
TAAQ (Teachers)hardo, A., Carvalho, B., Massano-Cardoso, I., Cunha, M. (2020). Assessing teacher-related experiential avoidance: Factor structure and psychometric properties of the Teachers Acceptance and Action Questionnaire (TAAQ-PT). International Journal of School & Educational Psychology,1-10. https://doi.org/10.1080/21683603.2020.1760978
Hinds, E., Jones, L. B., Gau, J. M., Forrester, K. K., & Biglan, A. (2015). Teacher distress and the role of experiential avoidance. Psychology in the Schools, 52(3), 284–297. https://doi.org/10.1002/pits.21821
TAAQ - Japanese
TAAQ - JapaneseKoh, Y., Iwasawa, N., Inoue, K., & Ohtsuki, T. (2024). Development and validation of a Japanese version of the Teachers Acceptance and Action Questionnaire. Journal of Contextual Behavioral Science, 31, 100726. DOI: 10.1016/j.jcbs.2024.100726
TAAQ - Portuguese
TAAQ - PortugueseCarvalho, B.A.F. & Galhardo, A. (2018) Questionário de Aceitação e Ação para Professores: desenvolvimento da versão portuguesa, estudo da estrutura fatorial e propriedades psicométricas. ISMT, Dissertation. The Portuguese TAAQ is in Appendix D.
TAQ (Tinnitus)
TAQ (Tinnitus)Tinnitus specific AAQ.
References:
Weise, C., Kleinstäuber, M., Hesser, H., Zetterqvist Westin, V. & Andersson, G. (2013). Acceptance of Tinnitus: Validation of the Tinnitus Acceptance Questionnaire. Cognitive Behaviour Therapy, 42(2), 100-115. DOI: 10.1080/16506073.2013.781670
Westin, V., Hayes, S. C., & Andersson, G. (2008). Is it the sound or your relationship to it? The role of acceptance in predicting tinnitus impact. Behaviour Research and Therapy, 46, 1259-1265. .
TAQ - Czech
TAQ - CzechKřenková, B. (2021). Vliv chronického tinnitu a míry jeho přijetí na vnímanou úroveň kognitivního výkonu. Thesis: Masarykova Univerzita. Retrieved from https://is.muni.cz/th/v4wyl/ The Czech version of Tinnitus Acceptance Questionnaire TAQ is in the Appendix.
TAQ - Japanese
TAQ - JapaneseTakabatake, S., Takahashi, M., Kabaya, K., Sekiya, Y., Sekiya, K., Harata, I., Kondo, M., et al. (2022). Validation of the Tinnitus Acceptance Questionnaire: Japanese Version. Audiology Research, 12(1), 66–76. http://doi.org/10.3390/audiolres12010006
VAAS (Auditory Hallucinations)
VAAS (Auditory Hallucinations)The Voices Acceptance and Action Questionnaire.
Reference: Shawyer, F., Ratcliff, K., Mackinnon, A., Farhall, J., Hayes, S.C. & Copolov, D. (2007). The voices acceptance and action scale (VAAS): Pilot data. Journal of Clinical Psychology, 63(6), 593–606.
VAAS - French
VAAS - FrenchLanglois T, Sanchez-Rodriguez R, Klein R, et al. (2020) [Acceptance of "voices" in people with or without psychiatric disorders: Francophone validation of the 9-item VAAS scale]. L'encephale,46(6):443-449. http://doi.org/10.1016/j.encep.2020.01.009
VAAS - Portuguese
VAAS - PortugueseMartins, M., Castilho, P., Macedo, A., Pereira, A., Vagos, P., Carvalho, D., Pascoal, C., & Carvalho, C. (2018). A pilot study of the Portuguese version of the Voices Acceptance and Action Scale: Psychometric properties in a clinical sample with psychosis-spectrum disorders. Analise Psicologica, 37(1). DOI: 10.14417/ap.1561
VAAS - Swedish
VAAS - SwedishUtvecklad av David Copolov mfl. Den svenska översättningen är gjord av Mårten Tyrberg, vid Psykosmottagningen Öster, Västmanlands Sjukhus, tillsammans med Sandra Bates och Tobias Lundgren.
Du hittar instrumentet här.
VAAS - Turkish
VAAS - TurkishMerve Terzioğlu*, K. Fatih Yavuz (2018) Turkish Version of Voices Acceptance and Action Questionnaire (VAAS): Preliminary Analysis of Reliability and Validity. Poster presented at ACBS World Conference 16.
WAAQ (work)
WAAQ (work)Bond, F. W., Lloyd, J., & Guenole, N. (2012). The work-related acceptance and action questionnaire (WAAQ): Initial psychometric findings and their implications for measuring psychological flexibility in specific contexts. Journal of Occupational and Organizational Psychology, 1-25.
For the full text of the article, follow this link: http://contextualscience.org/WAAQ_Bond_Lloyd_Guenola
Use of the WAAQ: Permission is hereby given to use the WAAQ for IRB/ethics-required research projects that occur in university and non-profit research institutions; in such cases, further author permission is not required. If, however, the WAAQ is to be used in any part of a money making enterprise (e.g., consultancy to organizations), the authors require that you seek their permission before using the measure. —Professor Frank Bond, Dr. Jo Lloyd, Goldsmiths College, University of London, 9, June 2020
WAAQ - Chinese
WAAQ - ChineseXu, X., Liu, X., Ou, M., Xie, C., & Chen Y.Z. (2018). Psychological flexibility of nurses in a cancer hospital: Preliminary validation of a chinese version of the work-related acceptance and action questionnaire. ASIA-PACIFIC JOURNAL OF ONCOLOGY NURSING, 5, 83-90. Available from: https://www.apjon.org/text.asp?2018/5/1/83/221482 The Chinese version of WAAQ is in Appendix 2.
WAAQ - Japanese
WAAQ - Japanese戸澤 杏奈, 松永 美希, 土屋 政雄, 中山 真里子, 熊野 宏昭 (2023 in press). 日本語版Work-related Acceptance and Action Questionnaire(WAAQ)の作成と信頼性・妥当性の検討. 認知行動療法研究. [Anna Tozawa, Miki Matsunaga, Masao Tsuchiya, Mariko Nakayama, Hiroaki Kumano (2023 in press). Development of a Japanese Version of the Work-related Acceptance and Action Questionnaire and Examination of Its Reliability and Validity. Japanese Journal of Behavioral and Cognitive Therapies.] DOI: 10.24468/jjbct.21-028
WAAQ - Portuguese
WAAQ - PortuguesePinto, V. N., Ferreira, M. C., & Valentini, F. (2015). Evidências de Validade da Escala de Flexibilidade Psicológica no Trabalho em Amostras Brasileiras. Psico, 46(3), 362-373. https://doi.org/10.15448/1980-8623.2015.3.18679 The Portuguese Escala de Flexibilidade Psicológica no Trabalho (WAAQ) is in the Appendix.
WAAQ - Spanish
WAAQ - SpanishReferences:
Bravo, D.M., Suárez-Falcón, J.C., Bianchi-Salguero, J.M., Gil-Luciano, B., & Ruiz, J. (2023). Psychometric properties and measurement invariance of the Work-Related Acceptance and Action Questionnaire (WAAQ) in a Colombian sample. International Journal of Psychology & Psychological Therapy, 23(3), 301-312. https://www.ijpsy.com/volumen23/num3/649.html
Ponce, M.C. & Villar, E. (2022). VALIDACIÓN DEL “CUESTIONARIO DE ACEPTACIÓN Y ACCIÓN LABORAL”(WAAQ) CON ESTUDIANTES UNIVERSITARIOS. Behavioral Psychology / Psicología Conductual, 30(1), 223-233. https://doi.org/10.51668/bp.8322111s
Ruiz, F. J., & Odriozola-González, P. (2014). Versión española del Cuestionario de Aceptación y Acción Relacionado con el Trabajo (WAAQ). Psicothema, 26(1).
WAAQ - Swedish
WAAQ - SwedishHolmberg, J. et al (2019). Evaluating the psychometric characteristics of the Work-related Acceptance and Action Questionnaire (WAAQ) in a sample of healthcare professionals. Journal of Contextual Behavioral Science, 14, 103-107. https://doi.org/10.1016/j.jcbs.2019.08.010
Abstract
The Work-related Acceptance and Action Questionnaire (WAAQ) has been developed to assess psychological flexibility in occupational settings. The aim of this study was to evaluate reliability and validity of the Swedish translation of WAAQ in a sample of 184 healthcare professionals. A principal component analysis supported a one-factor-solution, explaining 53.8% of the overall multivariate variability. WAAQ showed good internal consistency (Cronbach's alpha 0.85) and good test-retest reliability (ICC = 0.85). Validity was assessed by analysing the relationship between WAAQ and other work-related constructs. Spearman's rank correlations illustrated a significant negative relationship between WAAQ and perceived stress and a significant positive correlation with work engagement. Results from the study are consistent with previous studies on WAAQ, supporting the use of the Swedish translation of the instrument among healthcare professionals.
WAAQ - Turkish
WAAQ - TurkishAydın, G., Aydın, Y. & Karacan Özdemir, N. (2020). İş Yaşamında Kabul ve Eylem Formu: Geçerlik ve Güvenirlik Çalışması [Work-Related Acceptance and Action Questionnaire: Reliability and Validity Study of Turkish Version]. Kariyer Psikolojik Danışmanlığı Dergisi, 3(1), 32-54.
Body Image Psychological Inflexibility Scale (BIPIS)
Body Image Psychological Inflexibility Scale (BIPIS)Callaghan, G.M., Sandoz, E.K., Darrow, S.M., & Feeney, T.K. (2015). The Body Image Psychological Inflexibility Scale: Development and psychometric properties. Psychiatry Research, 226(1), 45-52. https://doi.org/10.1016/j.psychres.2014.11.039
BIPIS - Korean
BIPIS - KoreanKim J-C. (2019) 신체상에 대한 심리적 경직성이 신체변형장애 증상에 미치는 영향 [The effect of psychological rigidity on body image on the symptoms of body dysmorphic disorder]. Thesis. The Korean BIPIS is in Table 3.
BIPIS - Persian
BIPIS - PersianAmiri, S. & Yaghoubi, A.. (2017) Psychometric Properties of Body Image Psychological Inflexibility Scale. Iranian Journal of Psychiatry and Clinical Psychology, 23 (1), 94-107. https://doi.org/10.18869/NIRP.IJPCP.23.1.94
Chronic Pain Acceptance Questionnaire (CPAQ)
Chronic Pain Acceptance Questionnaire (CPAQ)McCracken, L.M., Vowles, K.E., & Eccleston, C. (2004) Acceptance of chronic pain: component analysis and a revised assessment method. Pain, 107(1–2), 159-166. https://doi.org/10.1016/j.pain.2003.10.012
Reneman, M.F., Dijkstra, A., Geertzen, J.H., & Dijkstra, P.U. (2010). Psychometric properties of Chronic Pain Acceptance Questionnaires: A systematic review. European Journal of Pain, 14, 457-465. DOI: 10.1016/j.ejpain.2009.08.003
CPAQ - Arabic
CPAQ - ArabicAl-Arfaj, S.K., Abdallah A.F., & Abdulla, F.A. (2023 in press). Psychometric properties of an Arabic translation of the chronic pain acceptance questionnaire (CPAQ) in a sample of patients with chronic pain. Disability and Rehabilitation. https://doi.org/10.1080/09638288.2023.2293987
CPAQ - Chinese
CPAQ - ChineseCheung MN, Wong TC, Yap JC, Chen PP. (2009) Validation of the Chronic Pain Acceptance Questionnaire (CPAQ) in Cantonese-speaking Chinese patients. J Pain, 9(9):823-32. https://doi.org/10.1016/j.jpain.2008.04.005
Liu, Y., Wang, L., Wei, Y., Wang, X., Xu, T., & Sun, J. (2016). Validation of a Chinese version of the Chronic Pain Acceptance Questionnaire (CAPQ) and CPAQ-8 in chronic pain patients. Medicine, 95(33), e4339. https://doi.org/10.1097/MD.0000000000004339
CPAQ - Czech
CPAQ - CzechKlocek, A., Řiháček, T., & Cígler, H. (2023). Measuring symptom acceptance: Psychometric evaluation of ‘chronic pain acceptance questionnaire – symptoms’ in a Czech clinical sample. Československá Psychologie, 67(1), 50-62. https://doi.org/10.51561/cspsych.67.1.50
CPAQ - Danish
CPAQ - Danishla Cour, P., & Højsted, J. (2015). Validation of the Danish-language chronic pain acceptance questionnaire. Acta anaesthesiologica Scandinavica, 59(10), 1377–1386. https://doi.org/10.1111/aas.12567
CPAQ - Finnish
CPAQ - FinnishOjala, T., Piirainen, A., Sipilä, K., Suutama, T., & Häkkinen, A. (2013). Reliability and validity study of the Finnish version of the Chronic Pain Acceptance Questionnaire (CPAQ). Disability and rehabilitation, 35(4), 306–314. https://doi.org/10.3109/09638288.2012.694572 The Finnish Translation of the CPAQ is in Appendix 1.
CPAQ - German Validation
CPAQ - German ValidationNilges, P., Köster, B. & Schmidt, C.O. (2007) Schmerzakzeptanz – Konzept und Überprüfung einer deutschen Fassung des Chronic Pain Acceptance Questionnaire. Schmerz, 21, 57–67. https://doi.org/10.1007/s00482-006-0508-1
CPAQ - Greek Validation
CPAQ - Greek ValidationVasiliou, V. S., Karekla, M., Michaelides, M. P., & Kasinopoulos, O. (2018). Construct validity of the G-CPAQ and its mediating role in pain interference and adjustment. Psychological Assessment, 30(2), 220–230. https://doi.org/10.1037/pas0000467
CPAQ - Italian Validation
CPAQ - Italian ValidationReferences:
Bernini, O., Rivas, T., & Berrocal, C. (2014). The Chronic Pain Acceptance Questionnaire: Preliminary evidence for the predictive validity of patients’ subgroups. Journal of Evidence-Based Psychotherapies, 14(1), 3–20.
Monticone M, Ferrante S, Rocca B, Nava T, Parini C, Cerri C. (2013). Chronic pain acceptance questionnaire: confirmatory factor analysis, reliability, and validity in Italian subjects with chronic low back pain. Spine, 38(13):E824-31. http://doi.org/10.1097/BRS.0b013e3182917299
Bernini, O., Pennato, T., Cosci, F., &Berrocal, C. (2010). The Psychometric Properties of the Chronic Pain Acceptance Questionnaire in Italian Patients with Chronic Pain. Journal of Health Psychology, 15(8):1236-1245. http://doi.org/10.1177/1359105310365576
CPAQ - Japanese
CPAQ - JapaneseTakaki Fukumori, Kengo Fujishima, Kazunori Iwasa, Yumiko Takao, Yukino Kobayashi, & Hiroyuki Nishie (2023). Validation of the Japanese version of the 8-item Chronic Pain Acceptance Questionnaire (CPAQ-8). The Journal of Medical Investigation, 70, 88-93. The Japanese version of the CPAQ-8 is in Table 1.
Kengo Fujishima, Takaki Fukumori, Stevetoshihisa Fukuda (2017) Development of the Japanese version of Chronic Pain Acceptance Questionnaire-8 (CPAQ-8J): In a sample of university students with chronic pain. The Proceedings of the Annual Convention of the Japanese Psychological Association, 2017, Volume 81, The 81st Annual Convention of the Japanese Psychological Association, Session ID 1B-033, Pages 1B-033. https://doi.org/10.4992/pacjpa.81.0_1B-033
CPAQ - Korean
CPAQ - KoreanCho, S., Heiby, E. M., McCracken, L. M., Moon, D. E., & Lee, J. H. (2012). Psychometric properties of a Korean version of the Chronic Pain Acceptance Questionnaire in chronic pain patients. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation, 21(6), 1059–1064. https://doi.org/10.1007/s11136-011-0010-9
CPAQ - Norwegian
CPAQ - NorwegianEide, H., Leren, L., & Sørebø, Ø. (2017). The Norwegian versions of the Chronic Pain Acceptance Questionnaire CPAQ-20 and CPAQ-8 - validation and reliability studies. Disability and rehabilitation, 39(14), 1441–1448. https://doi.org/10.1080/09638288.2016.1198427
CPAQ - Persian
CPAQ - PersianMesgarian, F; Asghari, A; Shaeiri, MR; Broumand, A. (2012). The Persian Version of the Chronic Pain Acceptance Questionnaire. Clinical Psychology and Psychotherapy. https://doi.org/10.1002/cpp.1769
Ebrahimi, A., Afshar-Zanjani, H., Goli, F., Rohafza, H. R., & Nasiri Dehsorkh, H. (2022). Psychometric Properties of the Persian Version of the Chronic Pain Acceptance Questionnaire in Patients with Chronic Pain in Isfahan, Tehran, and Yazd, Iran. International Journal of Body, Mind and Culture, 8(1), 65-74. Retrieved from https://ijbmc.org/index.php/ijbmc/article/view/251
CPAQ - Portuguese
CPAQ - PortugueseCosta, J. & Pinto Gouveia, J. (2009). Aceitação da dor. Abordagem do Chronic Pain Accepatnce Questionnaire (McCracken, Vowles & Eccleston, 2004) na população portuguesa com dor. Revista Psicologia, 23(1), 103-126.
CPAQ - Russian
CPAQ - Russian CommunityCPAQ - Spanish
CPAQ - SpanishRodero, B., García-Campayo, J., Casanueva, B., del Hoyo, Y. L., Serrano-Blanco, A., & Luciano, J. V. (2010). Validation of the Spanish version of the Chronic Pain Acceptance Questionnaire (CPAQ) for the assessment of acceptance in fibromyalgia. Health and quality of life outcomes, 8, 37. https://doi.org/10.1186/1477-7525-8-37
Sánchez-Rodríguez, E., de la Vega, R., Racine, M., Roy, R., Jensen, M. P., & Miró, J. (2019). Support for the Spanish version of the CPAQ-8 as a measure of chronic pain acceptance. Journal of evaluation in clinical practice, 25(5), 881–888. https://doi.org/10.1111/jep.13092
CPAQ - Swedish
CPAQ - Swedish CommunityCPAQ 20 items - Swedish
CPAQ 20 items - SwedishThe Chronic Pain Acceptance Questionnaire (CPAQ) avser att mäta acceptans av långvarig smärta och inkluderar två skalor: Activities engagement och Pain willingness. Activities engagement handlar om att utföra betydelsefulla aktiviteter oavsett smärtan. Formuläret är utvecklat av Lance McCracken och medarbeteare. Den svenska versionen är översatt av Rikard Wiksell och medarbetare. Du hittar instrumentet här.
Referenser:
[1] Wicksell RK, Olsson GL & Melin L . (2009) The Chronic Pain Acceptance Questionnaire (CPAQ)-further validation including a confirmatory factor analysis and a comparison with the Tampa Scale of Kinesiophobia. European Journal of Pain, 13, 760–768. Se artikeln här.
[2] McCracken, L.M., Vowles, K.E. & Eccleston, C. (2004). Acceptance of chronic pain: component analysis and a revised assessment method. Pain, 107, 159-66. Se artikeln här.
CPAQ-8 - Swedish
CPAQ-8 - SwedishRovner, G.; Årestedt, K.; Gerdle, B.; Börsbo, B. & McCracken, L.M. (2014). Psychometric properties of the 8-item Chronic Pain Acceptance Questionnaire (CPAQ - 8) in a Swedish Chronic Pain Cohort. Journal of Rehabilitation Medicine, 46(1), 73-80. Se artikeln här.
CPAQ - Turkish
CPAQ - TurkishHazel Ekin Akmaz, Meltem Uyar, Yasemin Kuzeyli Yıldırım, Esra Akın Korhan (2018). Validity and Reliability of the Turkish Chronic Pain Acceptance Questionnaire. Balkan Medical Journal, 35(3), 238-244. DOI: 10.4274/balkanmedj.2016.1998
Zure, M., Menekşeoğlu, A.K., & Ketenci, A. (2023). Validation of the Turkish Chronic Pain Acceptance Questionnaire-8. Turkish Journal of Physical Medicine & Rehabilitation, 69(x), i-vi. DOI: 10.5606/tftrd.2023.10857
CPAQ Excel Scoring File
CPAQ Excel Scoring FileI created this simple little excel file to automate the scoring of the CPAQ. Just input the raw ratings & it take care of the reverse scoring & summing.
I hope you find it useful.
~Scott Rower
Chronic Tinnitus Acceptance Questionnaire (CTAQ)
Chronic Tinnitus Acceptance Questionnaire (CTAQ)The Chronic Tinnitus Acceptance Questionnaire (CTAQ) is a 20-item self-report assessment adapted from the Chronic Pain Acceptance Questionnaire (CPAQ).
References:
Moreland, J. E. N. (2007). Illness Representations, Acceptance, Coping and Psychological Distress in Chronic Tinnitus. University of Leicester. Thesis. https://hdl.handle.net/2381/9098 The CTAQ is in the Appendix.
Moschen, R., et al (2019). Validation of the Chronic Tinnitus Acceptance Questionnaire (CTAQ-I): the Italian version. ACTA Otorhinolaryngologica Italica, 39(2). DOI: 10.14639/0392-100X-2144
Riedl, D., Rumpold, G., Schmidt, A., Zorowka, P. G., Bliem, H. R., & Moschen, R. (2015). The influence of tinnitus acceptance on the quality of life and psychological distress in patients with chronic tinnitus. Noise & health, 17(78), 374–381. https://doi.org/10.4103/1463-1741.165068
CTAQ - German
CTAQ - GermanReferences:
Riedl, D., Rumpold, G., Schmidt, A., Zorowka, P. G., Bliem, H. R., & Moschen, R. (2015). The influence of tinnitus acceptance on the quality of life and psychological distress in patients with chronic tinnitus. Noise & health, 17(78), 374–381. https://doi.org/10.4103/1463-1741.165068
CTAQ - Italian
CTAQ - ItalianMoschen, R., et al (2019). Validation of the Chronic Tinnitus Acceptance Questionnaire (CTAQ-I): the Italian version. ACTA Otorhinolaryngologica Italica, 39(2). DOI: 10.14639/0392-100X-2144
Hearing Acceptance Questionnaire (HAQ)
Hearing Acceptance Questionnaire (HAQ)The HAQ measures psychological acceptance among individuals with hearing problems.
Molander, P., Andersson, G., & Hesser, H. (2022). Psychological Acceptance in Adults With Hearing Loss—Psychometric Evaluation and Validation of the Hearing Acceptance Questionnaire. Ear and Hearing, 43(6), 1752-1760. DOI: 10.1097/AUD.0000000000001245
HAQ - Swedish
HAQ - SwedishMolander, P., Andersson, G., & Hesser, H. (2022). Psychological Acceptance in Adults With Hearing Loss—Psychometric Evaluation and Validation of the Hearing Acceptance Questionnaire. Ear and Hearing, 43(6), 1752-1760. DOI: 10.1097/AUD.0000000000001245
Psychological Flexibility in Epilepsy Questionnaire (PFEQ)
Psychological Flexibility in Epilepsy Questionnaire (PFEQ)Burket, L., Parling, T., Jansson-Fröjmark, M., Reuterskiöld, L., Ahlqvist, J., Shanavazh, S., Reinebo, G., Vinnars, B., Beckman, M., Bohman, B., Rozenthal, A., Larsson, C., Lindgren, A., Linde, J., Bonnert, M., & Lundgren, T. (2021). Development and preliminary evaluation of the psychometric properties of the psychological flexibility in epilepsy questionnaire (PFEQ). Epilepsy & Behavior, 115, 107685. https://doi.org/10.1016/j.yebeh.2020.107685
PFEQ - Persian
PFEQ - PersianDavoudi, M., Lundgren, T., Jansson-Fröjmark, M., Saeedipour, Z., & Badinlou, F. (2022). The Psychological Flexibility in Epilepsy Questionnaire (PFEQ): Psychometric properties of the Persian version. Epilepsy & Behavior, 130, 108672. https://doi.org/10.1016/j.yebeh.2022.108672
Psychological Inflexibility Scale – Infertility (PIS-I)
Psychological Inflexibility Scale – Infertility (PIS-I)Galhardo, A., Cunha, M., Monteiro, B, & Pinto-Gouveia, J. (2020). Assessing psychological inflexibility in infertility: The development and validation study of the Psychological Inflexibility Scale – Infertility (PIS-I). Journal of Contextual Behavioral Science, 18, 239-246. https://doi.org/10.1016/j.jcbs.2020.09.006 The scale is in Table 1.
PIS-I - Portuguese
PIS-I - PortugueseGalhardo, A., Cunha, M., Monteiro, B, & Pinto-Gouveia, J. (2020). Assessing psychological inflexibility in infertility: The development and validation study of the Psychological Inflexibility Scale – Infertility (PIS-I). Journal of Contextual Behavioral Science, 18, 239-246. https://doi.org/10.1016/j.jcbs.2020.09.006
Psychological Inflexibility in Pain Scale (PIPS)
Psychological Inflexibility in Pain Scale (PIPS)The Psychological Inflexibility in Pain Scale (PIPS) assesses both avoidance of pain and cognitive fusion with pain.
References:
Wicksell, R. K., Renöfält, J., Olsson, G. L., Bond, F.W. & Melin, L. (2008). Avoidance and cognitive fusion - central components in pain related disability? Development and preliminary validation of the Psychological Inflexibility in Pain Scale (PIPS). European Journal of Pain, 12, 491-500.
Vasiliou, V. S., Michaelides, M. P., Kasinopoulos, O., & Karekla, M. (2019). Psychological Inflexibility in Pain Scale: Greek adaptation, psychometric properties, and invariance testing across three pain samples. Psychological Assessment, 31(7), 895–904. https://doi.org/10.1037/pas0000705
PIPS - Chinese Version
PIPS - Chinese VersionXie CJ, Xu XH, Ou MJ, & Chen YY (2021). Chinese Version of the Psychological Inflexibility in Pain Scale for Cancer Patients Reporting Chronic Pain. Cancer Nursing, 44(3):180-189. https://doi.org/10.1097/ncc.0000000000000772
The Chinese Translation of the PIPS scale is at the end of the article.
PIPS - Dutch
PIPS - DutchBufink, Shanna (2009) A qualitative analysis of three pain scales translated into Dutch: The Psychological Inflexibility Pain Inventory, The Brief Pain Coping Inventory-2, The Brief Pain Response Inventory. Thesis: University of Twente. The Dutch PIPS translation final version is in the Attachments. Retrieved from http://essay.utwente.nl/59350/1/scriptie_S_Bufink.pdf
PIPS - French
PIPS - FrenchMartel, M.E., Dionne, F., Gauchet, A. et al (2015) Psychological inflexibility for pain: Translation and validation for a French-speaking population. Poster presented at ACBS Annual World Conference 13. The PIPS items are translated to French.
PIPS - German
PIPS - GermanBarke, A., Riecke, J., Rief, W. et al. (2015). The Psychological Inflexibility in Pain Scale (PIPS) – validation, factor structure and comparison to the Chronic Pain Acceptance Questionnaire (CPAQ) and other validated measures in German chronic back pain patients. BMC Musculoskelet Disord, 16, 171. https://doi.org/10.1186/s12891-015-0641-z The German version of the PIPS is in the article's "Additional File."
PIPS - Greek Adaptation
PIPS - Greek AdaptationVasiliou, V. S., Michaelides, M. P., Kasinopoulos, O., & Karekla, M. (2019). Psychological Inflexibility in Pain Scale: Greek adaptation, psychometric properties, and invariance testing across three pain samples. Psychological Assessment, 31(7), 895–904. https://doi.org/10.1037/pas0000705
Vasiliou, V. S. (2017). Acceptance and commitment therapy for primary headache sufferers : a randomized controlled trial. Dissertation: University of Cyprus. Retrieved from https://gnosis.library.ucy.ac.cy/handle/7/39514 The Greek PIPS-II is in Appendix B.
PIPS - Italian
PIPS - ItalianPsychological Inflexibility in Pain Scale (PIPS)
Wicksell, R. K., Renöfält, J., Olsson, G. L., Bond, F.W. & Melin, L. (2008). Avoidance and cognitive fusion - central components in pain related disability? Development and preliminary validation of the Psychological Inflexibility in Pain Scale (PIPS). European Journal of Pain, 12, 491-500.
Versione Italiana (1.0) a cura di Ristè, N., Lijoi, E., Rossi, E., Violini, P., Melchiorri, E., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Lijoi, E., Ristè, N. Melchiorri, E., Rossi, E., Violini, P., Panzera, A.,(2014). Avoidance and cognitive fusion in mental suffering: Adaptation and validation study of an Italian version of the Psychological Inflexibility in Pain Scale (PIPS) in Italian adolescents with psychological distress (2014). Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
PIPS - Japanese
PIPS - JapaneseNagasawa, Y., Shibata, A., Fukamachi, H., et al. (2021). The Psychological Inflexibility in Pain Scale (PIPS): Validity and Reliability of the Japanese Version for Chronic Low Back Pain and Knee Pain. Journal of Pain Research, 14, 325-332. http://doi.org/10.2147/jpr.s287549
PIPS - Persian
PIPS - PersianAbdollah Omidi, Zahra Zanjani, Mohammad Hosein Fadavi Kashani, Reza Daneshvar Kakhki (2018) The Evaluation of the Construct and Convergent Validity and Reliability of Psychological Inflexibility in Pain Scale in Individuals With Migraine Headache. Iranian Journal of Psychiatry and Behavioral Sciences, 12(3), e63132. DOI : 10.5812/ijpbs.63132
Ghomian S, Shairi MR, Masumian S, et al. (2017). Psychometric feature of the child and parent versions of Psychological Inflexibility in Pain Scale (PIPS) in children with chronic pain and their parents. Caspian J Pediatr, 3(2), 241-7.
PIPS - Portuguese
PIPS - PortugueseFerreirinha, C. & Galhardo, A. (2018) Estudo da Versão Portuguesa da Psychological Inflexibility in Pain Scale em Mulheres com Diagnóstico de Endometriose. ISMT, Dissertation. The Portuguese PIPS is in Appendix D.
PIPS - Spanish Validation
PIPS - Spanish ValidationRodero, B., Pereira, J. P., Pérez-Yus, M. C., Casanueva, B., Serrano-Blanco, A., Rodrigues da Cunha Ribeiro, M. J., Luciano, J. V., & Garcia-Campayo, J. (2013). Validation of a Spanish version of the psychological inflexibility in pain scale (PIPS) and an evaluation of its relation with acceptance of pain and mindfulness in sample of persons with fibromyalgia. Health and quality of life outcomes, 11, 62. https://doi.org/10.1186/1477-7525-11-62
PIPS - Swedish
PIPS - SwedishInstrumentet mäter psykologisk inflexibilitet vid smärttillstånd och är utvecklat av Rikard Wiksell och medarbetare vid Sektionen för Beteendemedicinsk Smärtbehandling, Smärtcentrum, Karolinska Universitetssjukhuset. Du hittar instrumentet här.
Referenser:
Wicksell, R. K., Renöfält, J., Olsson, G. L., Bond, F. W., & Melin, L. (2008). Avoidance and cognitive fusion--central components in pain related disability? Development and preliminary validation of the Psychological Inflexibility in Pain Scale (PIPS). European journal of pain (London, England), 12(4), 491–500. https://doi.org/10.1016/j.ejpain.2007.08.003
Wicksell, R.K., Ahlqvist, J., Bring, A., Melin, L., & Olsson, G.L. (2008). Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial. Cognitive Behavior Therapy, 37(3):169- 182. Se artikeln här.
Wicksell, R.K., Lekander, M., Sorjonen, K., & Olsson, G.L. (2010). The Psychological Inflexibility in Pain Scale (PIPS) – statistical properties and model fit of an instrument to assess change processes in pain related disability. European Journal of Pain, 14, e1-e14. Se artikeln här.
Wicksell, R.K., Olsson, G.L., & Hayes, S.C. (2010). Psychological flexibility as a mediator of improvement in Acceptance and Commitment Therapy for patients with chronic pain following whiplash. European Journal of Pain, 41, 1059.e1-1059.e11. Se artikeln här.
Wicksell, R.K., Renofalt, J., Olsson, G.L., Bond, F.W., & Melin, L. (2008). Avoidance and cognitive fusion-central components in pain related disability? Development and preliminary validation of the Psychological Inflexibility in Pain Scale (PIPS). European Journal of Pain, 12(4):491-500. Se artikeln här.
Values Measures
Values MeasuresThere is a systematic review of Values Measures in the Journal of Contextual Behavioral Science. ACBS members can read the full text of the article for free. Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304.
Bull's Eye Values Survey (BEVS)
Bull's Eye Values Survey (BEVS)This Bull's Eye is an approach developed by Tobias Lundgren and JoAnne Dahl at the University of Uppsala and successful used in a recent study on reducing epileptic seizures with ACT.
The Bulls-Eye 2 is the revised version of the measure and is currently being validated.
References:
Lundgren, T., Luoma, J.B., Dahl, J., Strosahl, K., &Melin, L. (2012). The Bull's-Eye Values Survey: A Psychometric Evaluation. Cognitive and Behavioral Practice, 19(4), 518-526. https://doi.org/10.1016/j.cbpra.2012.01.004
Barrett, K., O’Connor, M. & McHugh, L. A. (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
Bull's Eye - German Translation
Bull's Eye - German TranslationBull's Eye auf deutsch: https://contextualscience.org/bulls_eye_auf_deutsch
Bull's Eye - Greek
Bull's Eye - GreekSavvides, S. N. (2014). Evaluating an acceptance and commitment therapy internet-based intervention for smoking cessation in young adults. Dissertation, University of Cyprus. Retrived from https://gnosis.library.ucy.ac.cy/handle/7/39519 The Greek Bull's Eye is in Appendix B.
Bull's Eye - Hebrew
Bull's Eye - HebrewBull's Eye in Hebrew - עין השור / בול פגיעה
Bull's Eye - Norwegian
Bull's Eye - NorwegianTom Østergaard, Tobias Lundgren, Robert D. Zettle, Nils Inge Landrø, & Vegard Øksendal Haaland (2020) Psychological Flexibility in Depression Relapse Prevention: Processes of Change and Positive Mental Health in Group-Based ACT for Residual Symptoms. Front. Psychol. https://doi.org/10.3389/fpsyg.2020.00528
Bull's Eye - Polish
Bull's Eye - PolishOko Byka (Bulls Eye Thomasa Lundgreana, tłumaczenie Vivian Fiszer)
(Login to your ACBS account to see the attachment)
Bull's Eye - Spanish
Bull's Eye - SpanishThis is my spanish translation of the Bull's Eye exercise.
Bull's Eye - Swedish
Bull's Eye - SwedishBull's Eye Values Survey (BEVS)
Utvecklat av Tobias Lundgren m fl. Du hittar instrumentet här.
Referenser:
[1] Lundgren, T., Luoma, J.B., Dahl, J., Strosahl, K., Melin, L. (2012). The Bull's-Eye Values Survey: A Psychometric Evaluation. Cognitive and Behavioral Practice, 19, 518-526.
Bull's-eye Instrument about valued life Primary Care Version (BULLI-PC)
Bull's-eye Instrument about valued life Primary Care Version (BULLI-PC)Bull's-eye Instrument about valued life Primary Care Version (BULLI-PC) is in the ACT Measures Packet.
Chronic Pain Values Inventory (CPVI)
Chronic Pain Values Inventory (CPVI)The CPVI is in the ACT Measures Packet
References:
McCracken, L.M. & Yang, S. (2006) The role of values in a contextual cognitive-behavioral approach to chronic pain. Pain, 23, 137–45. https://doi.org/10.1016/j.pain.2006.02.021
Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
CPVI - Korean
CPVI - KoreanHaesol Hwang, Hwang & Janghan Lee. (2012) A study on the validity of the Korean version of the value test for chronic pain patients. Validation of the Korean Version of the Chronic Pain Values Inventory. Journal of The Korean Data Analysis Society, 14(5), 2499 - 2512.
CPVI - Swedish
CPVI - SwedishÅkerblom, S., Perrin, S., Fischer, M. R., & Mccracken, L. M. (2017). Further validation of the Chronic Pain Values Inventory in a Swedish chronic pain sample. Journal of Contextual Behavioral Science, 6(3), 261-267. doi:10.1016/j.jcbs.2017.06.001
Engaged Living Scale (ELS)
Engaged Living Scale (ELS)References:
Trompetter, H. R., ten Klooster, P. M., Schreurs, K. M. G., Fledderus, M., Westerhof, G. J., & Bohlmeijer, E. T. (2013). Measuring values and committed action with the Engaged Living Scale (ELS): Psychometric evaluation in a nonclinical sample and a chronic pain sample. Psychological Assessment, 25(4), 1235–1246. https://doi.org/10.1037/a0033813
Barrett, K., O’Connor, M. & McHugh, L. A. (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
Spencer, S.D., Jo, D., Hamagami F., Antonio, M.C.K., Qinaʻau, J., Masuda, A., & Hishinuma, E.S. (2022). A psychometric validation of contextual cognitive behavioral therapy-informed measures with racially and ethnically diverse adults. Journal of Contextual Behavioral Science. https://doi.org/10.1016/j.jcbs.2022.06.004
ELS - Chinese
ELS - ChineseYang, Y. (2022). Cross-cultural adaptation and validation of the core psychometric instruments used in acceptance and commitment therapy (ACT): assessing the validity and reliability of ACT measures in the Chinese populations. Disseration, University of Edinburgh. http://dx.doi.org/10.7488/era/2645
ELS - Dutch
ELS - DutchEngaged Living Scale (ELS) - Dutch https://www.acbsbene.com/documenten-downloads/assessment/engaged-living-scale-els/
References:
Mislim, Rana (2013) Het meten van waardengericht leven: Validering van de Engaged Living Scale. Thesis: Universiteit Twente.
ELS - Korean
ELS - KoreanSeran Park (2020) Validation of Korean Version of Engaged Living Scale. Humanities and Social Sciences 21, Vol. 11, No. 2, 225-240.
ELS - Norwegian
ELS - NorwegianTom Østergaard, Tobias Lundgren, Robert D. Zettle, Nils Inge Landrø, & Vegard Øksendal Haaland (2020) Psychological Flexibility in Depression Relapse Prevention: Processes of Change and Positive Mental Health in Group-Based ACT for Residual Symptoms. Front. Psychol. https://doi.org/10.3389/fpsyg.2020.00528
ELS - Portuguese
ELS - PortugueseTrindade, I. A., Ferreira, C., Pinto-Gouveia, J., & Nooren, L. (2016). Clarity of personal values and committed action: Development of a shorter Engaged Living Scale. Journal of Psychopathology and Behavior Assessment, 38(2), 258-265. doi: 10.1007/s10862-015-9509-7
ELS - Spanish
ELS - SpanishNavarrete, J. Et Al (2023 in press). Psychometric properties of the engaged living scale (ELS) Spanish version in a large sample of Spanish pilgrims. Journal of Contextual Behavioral Science. https://doi.org/10.1016/j.jcbs.2023.05.001
ELS - Turkish
ELS - TurkishReferences:
Işık, H. R. & Bilge, Y. (2023) Değerlere Bağlı Yaşam Ölçeği: Türk Kültürüne Uyarlama Geçerlik ve Güvenirlik Çalışması. [Engaged Living Scale: The Study of Validity and Reliability and Adaptation to Turkish Culture.] Journal of Cognitive-Behavioral Psychotherapy and Research, 12(2), 145-155. doi:10.5455/JCBPR.112588
Valued Living Questionnaire (VLQ)
Valued Living Questionnaire (VLQ)The Valued Living Questionnaire is a simple questionnaire originally developed as a clinical tool. It's categories map relatively closely to the categories in the original ACT book (no surprise, since I authored both). A copy of the paper is available by clicking the citation below.
Wilson, K. G., Sandoz, E. K., Kitchens, J., & Roberts, M. E. (2010). The Valued Living Questionnaire: Defining and measuring valued action within a behavioral framework. The Psychological Record, 60, 249-272.
The manuscript contains a copy of the VLQ. I have also added a short working guide to its use.
Also, to get additional info on the flavor of the values work, I would recommend reading my chapter with Amy Murrell in the Mindfulness and Acceptance book. The chapter is also available here on this site: Values Work in ACT.
peace all,
Kelly Wilson
The VLQ can be found on stevenchayes.com
There is a VLQ Adapted to Caregiving (VLQAC) version.
References:
Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
Barrett, K., O’Connor, M. & McHugh, L. A. (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
VanBuskirk, K., West, L., Malcarne, V. et al. (2012). Confirmatory Factor Analysis of the Valued Living Questionnaire in a Black American Sample: Implications for Cognitive Research and Practice. Cognitive Therapy and Research, 36, 796-805. https://doi.org/10.1007/s10608-011-9405-8
Wilson, K. G., Sandoz, E. K., Kitchens, J., & Roberts, M. E. (2010). The Valued Living Questionnaire: Defining and measuring valued action within a behavioral framework. The Psychological Record, 60, 249-272.
VLQ - Arabic
VLQ - ArabicAdel, S. (2019). فعالية برنامج عالجي بالتقبل وااللتزام لتحسين صورة الجسم لدى عينة من ذوات اضطراب الشره العصبى [Efficacy of ACT program to improve body image for Female Bulimia nervosa disorder]. Thesis: University of Alexandria. The Arabic VLQ-2 is in the appendix.
VLQ - Brazilian Portuguese version
VLQ - Brazilian Portuguese versionCarolina Rodrigues Jesus Fernandes (2012) Validação da versão portuguesa da Escala de Valores numa amostra de estudantes universitários [Validation of the Portuguese version of the Valued Living Questionnaire in a sample of college students]. Universidade de Coimbra, Dissertação.
VLQ Brazilian version (See attachment below) Corresponding author: Paola Lucena-Santos, Ph.D. in Clinical Psychology. E-mail: paolabc2.lucena@gmail.com WhatsApp: +55 (51) 998055874 Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
VLQ - Czech
VLQ - CzechPetříková, K. (2021). Atributy acceptance and commitment therapy (ACT) v kontextu syndromu vyhoření u studentů medicíny. Thesis: Masarykova Univerzita. Retrieved from https://is.muni.cz/th/ww25y/ The Czech version of VLQ is in the Appendix.
VLQ - Greek
VLQ - GreekDafne Morroni, Vasilis S. Vasiliou & Maria Karekla (2020) Psychometric Properties of the Valued Living Questionnaire-Greek version (VLQ-G). Poster presented at the ACBS Annual World Conference 18.
VLQ - Hungarian
VLQ - HungarianSzabó, Vanda Virág and Gergely, Bence and Szabó-Bartha, Anett (2020). Az értékvezérelt élet kérdőív (VLQ) Magyar változatának pszichometriai jellemzői. Psychologia Hungarica Caroliensis, 8(2), 49-67. Retrieved from http://real.mtak.hu/id/eprint/143516 Következtetések: Végeredményben a teszt tartalma nehezen megragadható. Az eredmények alapján a teszt további használata hibás eredményekhez vezethet, így ez csak különös körültekintéssel ajánlható.
VLQ - Italian
VLQ - ItalianVLQ - Japanese
VLQ - JapaneseMorimoto H, Kishita N, Kondo H, Muto T. (2023). Reliability and validity of the Japanese version of the Valued Living Questionnaire Adapted to Caregiving. Clinical Gerontologist. http://doi.org/10.1080/07317115.2022.2163951.
VLQ - Korean
VLQ - KoreanPark Se-Ram, Lee Hoon-Jin (2012) ACT 기반 가치탐색 집단 프로그램의 효과연구 [The Effect of the ACT-Based Value Exploration Program on Valued Living and Psychological Adjustment]. Cognitive Behavior Therapy in Korea, 12(1), 1-20.
VLQ - Persian
VLQ - PersianMEHDI, A. (2018) The Reliability and Validity of Persian version of the Valued Living Questionnaire: based on Acceptance and Commitment approach. CLINICAL PSYCHOLOGY & PERSONALITY (DANESHVAR RAFTAR), Volume 16, Number 1 (30), 239 To 249. https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=741926
VLQ - Spanish
VLQ - SpanishRomero-Moreno, R., Gallego-Alberto, L., Márquez-González, M. & Losada, A. (2017). Psychometric properties of the Valued Living Questionnaire Adapted to Dementia Caregiving. Aging & Mental Health, 21(9), 983-990. DOI: 10.1080/13607863.2016.1191055
The VLQ Spanish Version can be found on Grupo ACT https://grupoact.com.ar/wp-content/uploads/2013/10/Cuestionario-de-valores-Importancia-y-consistencia-argentino.pdf
VLQ - Turkish
VLQ - TurkishReferences:
Çekici, F., Aydın-Sünbül, Z., Malkoç, A., Aslan Gördesli, M., & Arslan, R. (2018). Değer odaklı yaşam ölçeği: Türk kültürüne uyarlama geçerlik ve güvenirlik çalışması. Electronic Turkish Studies, 13(19), 459–471. https://doi.org/10.7827/TurkishStudies.14094
M. Emrah Karadere, Hasan Turan Karatepe, Kaasım Fatih Yavuz, Sevinc Ulusoy, Alparslan Cansız, Murat Aktepe (2017) Turkish Version of Valued Living Questionnaire (VLQ): Preliminary Analysis of Reliability and Validity in Non-Clinical Sample. Poster presented at ACBS World Conference 15.
Hasan Turan Karatepe, M. Emrah Karadere, Kaasım Fatih Yavuz, Sevinc Ulusoy, Murat Aktepe, Alparslan Cansız (2017) Turkish Version of Valued Living Questionnaire (VLQ): Preliminary Analysis of Reliability and Validity in Bipolar Disorder and Schizophrenia Sample. Poster presented at ACBS World Conference 15.
Valuing Questionnaire (VQ)
Valuing Questionnaire (VQ)The Valuing Questionnaire (VQ) is attached below.
References:
Smout, M., Davies, M., Burns, N., & Christie, A. (2014). Development of the Valuing Questionnaire (VQ). Journal of Contextual Behavioral Science, 3(3), 164–172. doi:10.1016/j.jcbs.2014.06.001
Full article available for ACBS members, logged in, here: https://contextualscience.org/article/development_of_the_valuing_questionnaire_vq
Barrett, K., O’Connor, M. & McHugh, L. A. (2019). Systematic Review of Values-Based Psychometric Tools Within Acceptance and Commitment Therapy (ACT). The Psychological Record, 69, 457–485. https://doi.org/10.1007/s40732-019-00352-7
Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
Kibbey, M.M, DiBello, A.M., Babu, A.A., & Farris, S.G. (2020). Validation of the Valuing Questionnaire (VQ) in adults with cardiovascular disease and risk. Journal of Contextual Behavioral Science, 17, 144-151. doi: 10.1016/j.jcbs.2020.07.006
Full article available for ACBS members, logged in, here: https://contextualscience.org/article/validation_of_the_valuing_questionnaire_vq_in_adults_with_cardiovascular_di
Aller, T.B., Barrett, T., Levin, M.E., McClain, M.B. (2022). Measuring psychological flexibility in autistic adults: Examining the validity and reliability of the AAQ-II, BEAQ, and VQ. Journal of Contextual Behavioral Science, 26, 125-133. DOI: 10.1016/j.jcbs.2022.09.001
Full article available for ACBS members, logged in, here: https://contextualscience.org/article/measuring_psychological_flexibility_in_autistic_adults_examining_the_validi
VQ - Chinese
VQ - ChineseBI Dandan, DING Qingwen, ZHANG Jiameng, CHEN Jie, LI Xinying (2021) Validity and reliability of the Chinese version of the Valuing Questionnaire in college students. Chinese Mental Health Journal, 5, 417-422. The article was retrieved from CAOD.
VQ - Greek
VQ - GreekVasiliou, V. S. (2017). Acceptance and commitment therapy for primary headache sufferers : a randomized controlled trial. Dissertation: University of Cyprus. Retrieved from https://gnosis.library.ucy.ac.cy/handle/7/39514 The Greek Valuing Questionnaire is in Appendix B.
VQ - Japanese
VQ - JapaneseThe Japanese version of Valuing Questionnaire (VQ) is a scale that measures the degree of life in line with value in a format that includes life areas for "value," which is the core process of ACT.
VQ is a 10-item 2-factor structure.
Rimi Doi, Asako Sakano, Takashi Muto, Yuji Sakano. (2017). Verification of the reliability and validity of the Japanese version of Valuing Questionnaire (VQ). Behavior Therapy Research, 43 (1), 83-94.
The VQ Japanese version is on the ACBS Japan Chapter website.
VQ - Korean
VQ - KoreanChoon-Ja Yoo, Kyung-Park Park. (2017) 한국판 가치질문지 타당화 연구 [A Validation Study of a Korean Version of Valuing Questionnaire(VQ)]. Korean Psychological Association Conference Materials, 2017 Annual Conference of the Korean Psychological Association, 2017.08, 313 - 313
Choonja Yoo, Ph.D., Kyung Park, Ph.D. (2018) A Validation Study of a Korean Version of Valuing Questionnaire(K-VQ). Poster presented at the ACBS World Conference 16.
VQ - Norwegian
VQ - NorwegianVQ norsk versjon oversatt og tilpasset av Eli Alperstein, Hans J Johansen mfl.. etter tillatelse fra Matthew Smout. Prosessnotater vedlegges i tråd med who oversettelsesprotokollen.
VQ - Persian
VQ - PersianNonahal S, Mohammadkhani S, Hasani J, Akbari M. (2020) Psychometric Properties of the Persian Version of the Valuing Questionnaire (VQ) in Population Engaging in Weight Loss. Journal of Research in Psychological Health, 14 (3), 1-17
URL: http://rph.khu.ac.ir/article-1-3671-en.html
OMIDI, A., & Ardestani, S., & HASSANABADI, H. (2018). Adaptation and Factor Structure of Valuing Questionnaire in Acceptance and Commitment Therapy Approach. TRAINING MEASUREMENT, 8(32), 85-101. https://dx.doi.org/10.22054/jem.2019.31526.1731
VQ - Polish
VQ - PolishBaran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego.
See attachments for male and female versions of the VQ. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
A different translation of the VQ: https://contextualscience.org/warto_cikwestionariuszzadanie_domowe
VQ - Portuguese
VQ - PortugueseReferences:
Carvalho, S.A., Palmeira, L., Pinto-Gouveia, J., Gillanders, D., & Castilho, P. (2018). The utility of the Valuing Questionnaire in Chronic Pain. Journal of Contextual Behavioral Science, 9, 21-29. https://doi.org/10.1016/j.jcbs.2018.06.002
Assaz, D.A. (2019) Desfusão cognitiva na Terapia de Aceitação e Compromisso(ACT): O processo de mudança clínica. UNIVERSIDADE DE SÃO PAULO, Dissertation. The Portuguese VQ is in Anexo K.
VQ - Spanish
VQ - SpanishRuiz, F. J., Suárez-Falcón, J. C., Segura-Vargas, M. A., & Gil-Luciano, B. (2021). Psychometric properties of the Spanish version of the Valuing Questionnaire in Colombian clinical and nonclinical samples. Journal of Clinical Psychology, 1– 16. https://doi.org/10.1002/jclp.23212
Ruiz, F. J., Odriozola-González, P., Suárez-Falcón, J. C., & Segura-Vargas, M. A. (2022). Psychometric properties of the Valuing Questionnaire in a Spaniard sample and factorial equivalence with a Colombian sample. PeerJ, 10, e12670. https://doi.org/10.7717/peerj.12670
VQ - Swedish
VQ - SwedishRickardsson, J., Zetterqvist, V., Kemani, M. K., Holmström, L., Andersson, E., & Wicksell, R. K. (2019). Assessing values – Psychometric properties of the Swedish version of the Valuing Questionnaire in adults with chronic pain. Journal of Contextual Behavioral Science, 14, 40-49. https://doi.org/10.1016/j.jcbs.2019.08.009
VQ - Turkish
VQ - TurkishAydın, Y., Aydın, G. (2017). Değer Verme Ölçeği (Valuing Questionnaire)’ni Türk kültürüne uyarlama çalışması. Abant İzzet Baysal Üniversitesi Eğitim Fakültesi Dergisi, 17 (1), 64-77. See article here.
Other ACT-Related Measures
Other ACT-Related MeasuresThis page is a working list of other measures related to ACT processes.
ACT Check
ACT CheckThe ACT Check is a test for Assessing Knowlege of Acceptance and Commitment Therapy. The ACT Check consists of two parts: a theoretical section with 28 items for assessing understanding of the psychological flexibility model and an advanced section with 24 items for assessing applied understanding of ACT and the psychological flexibility model. (The original version is in Japanese.)
井上 和哉, 新堂 光太郎, 村松 穂香, 林 幹浩, & 大月 友. (2022). Acceptance and Commitment Therapy: ACT理解度テスト(ACT Check)の作成の試み. 行動医学研究, 27(1), 39-51. [Kazuya Inoue, Kotaro Shindo, Honoka Muramatsu, Mikihiro Hayashi, & Tomo Otsuki. (2022). Developing a Test for Assessing Knowlege of Acceptance and Commitment Therapy. Japanese Journal of Behavioral Medicine, 27(1), 39-51.] DOI: 10.11331/jjbm.27.39
ACT Knowledge Questionnaire
ACT Knowledge QuestionnaireThe ACT Knowledge Questionnaire is a 16 item measure of conceptual knowledge of ACT for use in studies and evaluation of the training of therapists who are learning ACT. It was original created for use in the following study:
- Luoma, J. B. & Plumb, J. (2013). Improving Therapist Psychological Flexibility While Training Acceptance and Commitment Therapy: A Pilot Study. Cognitive Behaviour Therapy 42(1), 1-8. DOI:10.1080/16506073.2012.701662
and has been used in the following published study:
- Richards, R., Oliver, J. E., Morris, E., Aherne, K., Iervolino, A. C., & Wingrove, J. (2011). Acceptance and Commitment Therapy training for clinicians: An evaluation. The Cognitive Behaviour Therapist, 4, 114-121.
The measure and scoring instructions are included in the attachment below (you need to be signed in to see it).
ACT session questionnaire (ACT-SQ)
ACT session questionnaire (ACT-SQ)The ACT-SQ is a short questionnaire capturing the patients’ view of the in-session realization of the six core components of Acceptance and Commitment Therapy (ACT).
References:
Probst, T., Mühlberger, A., Kühner, J., Eifert, G. H., Pieh, C., Hackbarth, T., & Mander, J. (2020). Development and Initial Validation of a Brief Questionnaire on the Patients’ View of the In-Session Realization of the Six Core Components of Acceptance and Commitment Therapy. Clinical Psychology in Europe, 2(3), 1-23. https://doi.org/10.32872/cpe.v2i3.3115 The ACT-SQ English version and German version is in the article's Supplementary Materials.
ACT-SQ - German
ACT-SQ - GermanProbst, T., Mühlberger, A., Kühner, J., Eifert, G. H., Pieh, C., Hackbarth, T., & Mander, J. (2020). Development and Initial Validation of a Brief Questionnaire on the Patients’ View of the In-Session Realization of the Six Core Components of Acceptance and Commitment Therapy. Clinical Psychology in Europe, 2(3), 1-23. https://doi.org/10.32872/cpe.v2i3.3115 The German version ACT-SQ is in the article's Supplementary Materials.
Acceptance and Commitment Therapy Fidelity Measure (ACT-FM)
Acceptance and Commitment Therapy Fidelity Measure (ACT-FM)Lucy O'Neill, Gary Latchford, Lance M. McCracken, Christopher D. Graham (2019). The development of the Acceptance and Commitment Therapy Fidelity Measure (ACT-FM): A delphi study and field test. Journal of Contextual Behavioral Science, 14, 111-118.
https://doi.org/10.1016/j.jcbs.2019.08.008 See attachment for the ACT-FM form.
ACT-FM - Spanish
ACT-FM - SpanishThe Medida de Fidelidad ACT (ACT-FM) can be found on Grupo ACT https://grupoact.com.ar/wp-content/uploads/2019/11/ACT-FMcastellano.pdf
Committed Action Questionnaire (CAQ)
Committed Action Questionnaire (CAQ)McCracken, L.M. (2013) Committed Action: An Application of the Psychological Flexibility Model to Activity Patterns in Chronic Pain. The Journal of Pain, 14(8), 828-835. https://doi.org/10.1016/j.jpain.2013.02.009
McCracken, L., Chilcot, J. & Norton, S. (2015). Committed action in chronic pain. Eur J Pain, 19, 677-685. https://doi.org/10.1002/ejp.589
CAQ - Dutch
CAQ - DutchKraiß, J.T. (2014) Measuring committed action : psychometric evaluation of the committed action questionnaire (CAQ) in a nonclinical sample. Retrieved from http://purl.utwente.nl/essays/65750 The CAQ-24 Dutch Translation is in the Appendix.
CAQ - German
CAQ - GermanTerhorst, Y., Baumeister, H., McCracken, L.M. et al. (2020). Further development in the assessment of psychological flexibility: validation of the German committed action questionnaire. Health and Quality of Life Outcomes, 18, 260. https://doi.org/10.1186/s12955-020-01497-8
CAQ - Swedish Validation
CAQ - Swedish ValidationÅkerblom S, Perrin S, Fischer MR, McCracken LM. (2016) A Validation and Generality Study of the Committed Action Questionnaire in a Swedish Sample with Chronic Pain. Int J Behav Med, 23(3):260-270. https://doi.org/10.1007/s12529-016-9539-x
CAQ-8 - Chinese
CAQ-8 - ChineseWong, W.-s., McCracken, L., Wong, S., Chen, P.-p., Chow, Y.-f., & Fielding, R. (2016). The Chinese version of the 8-item Committed Action Questionnaire (ChCAQ-8): A preliminary analysis of the factorial and criterion validity. Psychological Assessment, 28(6), e111–e118. https://doi.org/10.1037/pas0000187
Li, Y., Yang, F. L., Pan, C., Chu, Q. Q., and Tang, Q. P. (2021). Validation of the committed action Questionnaire-8 and its mediating role between experiential avoidance and life satisfaction among Chinese university students. Front. Psychol. 12, 655518. DOI: 10.3389/fpsyg.2021.655518
CAQ-8 - French
CAQ-8 - FrenchJoel Gagnon, Frédérick Dionne, Marcos Balbinotti, & Jean-Louis Monestès (2017). Dimensionality and validity of the Committed Action Questionnaire (CAQ-8) in a chronic pain and university student population. Journal of Contextual Behavioral Science, 6(3), 252-260. https://doi.org/10.1016/j.jcbs.2017.06.002 French Translation is in Table 1.
CAQ-8 - Greek
CAQ-8 - GreekVasiliou, V. S. (2017). Acceptance and commitment therapy for primary headache sufferers : a randomized controlled trial. Dissertation: University of Cyprus. Retrieved from https://gnosis.library.ucy.ac.cy/handle/7/39514 The Greek Committed Action Questionaire is in Appendix B.
CAQ-8 - Korean
CAQ-8 - KoreanPark Y-S, et al. (2016) Validation of Korean Version of a Shortened Committed Action Questionnaire(KCAQ-8). Korean Journal of Health Psychology, 21(3), 593-606. https://doi.org/10.17315/kjhp.2016.21.3.007
CAQ-8 - Persian
CAQ-8 - PersianMazloom M, Mohammadkhani S, Akbari M, & Hasani J. (2020). Psychometric Properties of the Committed Action Questionnaire, the Persian Version. Practice in Clinical Psychology, 8(2), 153-162. URL: http://jpcp.uswr.ac.ir/article-1-677-en.html
CAQ-8 - Polish
CAQ-8 - PolishBaran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
See attachments for male and female versions of the CAQ-8.
CAQ-8 - Portuguese
CAQ-8 - PortugueseTrindade, I. A., Marta-Simões, J., Ferreira, C., & Pinto-Gouveia, J. (2018). Developments on committed action: Validity of the CAQ-8 and analysis of committed action’s role in depressive symptomatology in breast cancer patients and healthy individuals. Clinical Psychology and Psychotherapy, 25(1), e42–e50. doi: 10.1002/cpp.2125
Rodrigues, T. F., Vieira, A. I., Vaz, A. R., Brandão, I., Timóteo, S., Nunes, P., Fernandez-Aranda, F., & Machado, P. P. P. (2022). The factorial structure and psychometric properties of the Committed Action Questionnaire (CAQ-8) in a Portuguese clinical sample with eating disorders. Clinical Psychology & Psychotherapy, 29(1), 222– 229. https://doi.org/10.1002/cpp.2621
CAQ-8 - Spanish
CAQ-8 - SpanishSánchez-Rodríguez, E, de la Vega, R, Racine, M, Roy, R, Jensen, MP, Miró, J. (2018). Support for the Spanish version of the CPAQ-8 as a measure of chronic pain acceptance. Journal of Evaluation in Clinical Practice, 25, 881– 888. https://doi.org/10.1111/jep.13092
Experiences Questionnaire (EQ)
Experiences Questionnaire (EQ)The EQ is a 20 item self-report scale designed to measure decentering and rumination.
Reference:
Fresco, D. M., Moore, M. T., van Dulmen, M., Segal, Z. V., Teasdale, J. D., Ma, H., & Williams, J. M. G. (2007). Initial psychometric properties of the Experiences Questionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38, 234-246. The EQ 20 items are in Table 1.
Please contact David Fresco if you would like to receive a copy of the measure.
EQ - German
EQ - GermanJudith Gecht, Ramona Kessel, Verena Mainz, Siegfried Gauggel, Barbara Drueke, Anne Scherer & Thomas Forkmann (2014). Measuring decentering in self-reports: Psychometric properties of the Experiences Questionnaire in a German sample. Psychotherapy Research, 24(1), 67-79. http://doi.org/10.1080/10503307.2013.821635
EQ - Japanese
EQ - JapaneseKURIHARA, Ai, HASEGAWA, Akira, & NEDATE, Kaneo (2011). Development of the Japanese Version of the Experiences Questionnaire and Examination of Its Reliability and Validity. Japanese Journal of Personality,19(2), 174-177.
EQ - Portuguese
EQ - PortugueseEQ Translation - see attachment
Corresponding author: Paola Lucena-Santos.
E-mail: paolabc2.lucena@gmail.com WhatsApp: +351 910391274
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
Address: Rua do Colégio Novo, Apartado 6153. Postal Code: 3001-802. Coimbra, Portugal.
References:
Gregório, S., Pinto-Gouveia, J., Duarte, C., & Simões, L. (2015). Expanding Research on Decentering as Measured by the Portuguese Version of the Experiences Questionnaire. The Spanish Journal of Psychology, 18, E23. doi:10.1017/sjp.2015.18
EQ - Spanish
EQ - SpanishSoler, J., Franquesa, A., Feliu-Soler, A., Cebolla, A., Carcia-Campayo, J., Tejedor, R., ... and Portella, M.J. (2014). Assessing decentering: Validation, psychometric properties and clinical usefulness of the Experiences Questionnaire in Spanish sample. Behavior Therapy, 45, 863-871. https://doi.org/10.1016/j.beth.2014.05.004
EQ - Turkish
EQ - TurkishÜnlü Kaynakçı, F . (2018). Merkezsizleştirme Becerisini Değerlendirme: Yaşantılar Ölçeğinin Türkçe Formunun Psikometrik Özellikleri [Measuring Decentering: Psychometric properties of the Turkish Version of Experiences Questionnaire]. Journal of Measurement and Evaluation in Education and Psychology, 9 (2), 150-160. DOI: 10.21031/epod.367560
Experiential Approach Scale (EAS)
Experiential Approach Scale (EAS)Swails, J.A., Zettle, R.D., Burdsal, C.A. et al. (2016). The Experiential Approach Scale: Development and Preliminary Psychometric Properties. The Psychological Record, 66, 527–545. https://doi.org/10.1007/s40732-016-0188-x
EAS - Spanish
EAS - SpanishReyes-Martín, S., Hernández-López, M., & Rodríguez-Valverde, M. (2021). Spanish Adaptation of the Experiential Approach Scale (EAS). International Journal of Environmental Research and Public Health, 18(24), 12873. DOI:10.3390/ijerph182412873 The EAS Spanish items are in Table 1.
Open and Engaged State Questionnaire (OESQ)
Open and Engaged State Questionnaire (OESQ)The OESQ is a brief, state-related self-report process measure of psychological flexibility.
References:
Benoy, C., Knitter, B., Knellwolf, L., Doering, S., Klotsche, J., & Gloster, A.T. (2019) Assessing psychological flexibility: Validation of the Open and Engaged State Questionnaire. Journal of Contextual Behavioral Science, 12, 253-260. https://doi.org/10.1016/j.jcbs.2018.08.005
Rogge, R.D., Daks, J.S., Dubler, B.A., & Saint, K.J. (2019) It's all about the process: Examining the convergent validity, conceptual coverage, unique predictive validity, and clinical utility of ACT process measures. Journal of Contextual Behavioral Science, 14, 90-102. https://doi.org/10.1016/j.jcbs.2019.10.001
Process-Based Assessment Tool (PBAT)
Process-Based Assessment Tool (PBAT)Download the PBAT at https://pbatsupport.com
References:
Ciarrochi, J., Hayes, S. C., & Hofmann, S. G. (2021). Assessing Processes of Change in Psychological Interventions: The Process-Based Assessment Tool (PBAT). PsyArXiv. https://doi.org/10.31234/osf.io/2pbcf The PBAT is in the appendix.
Ciarrochi, J., Sahdra, B., Hofmann, S., & Hayes, S. C. (2022). Developing an item pool to assess processes of change in psychological interventions: The Process-Based Assessment Tool (PBAT). Journal of Contextual Behavioral Science, 23, 200-213. DOI: 10.1016/j.jcbs.2022.02.001
Sanford, B.T., Ciarrochi, J., Hofmann, S.G., Gates, K.M., & Hayes, S.C. (2022). Toward empirical process-based case conceptualization: An idionomic network examination of the process-based assessment tool. Journal of Contextual Behavioral Science, 25, 10-25. https://doi.org/10.1016/j.jcbs.2022.05.006
PBAT - German
PBAT - GermanThe PBAT German translation is at https://pbatsupport.com/free-download/
PBAT - Italian
PBAT - ItalianThe PBAT Italian translation is at https://pbatsupport.com/free-download/
Self Experiences Questionnaire (SEQ)
Self Experiences Questionnaire (SEQ)SEQ: Yu, L., McCracken, L.M. & Norton, S. (2016). The Self Experiences Questionnaire (SEQ): Preliminary analyses for a measure of self in people with chronic pain. Journal of Contextual Behavioral Science, 5(3), 127-133. https://doi.org/10.1016/j.jcbs.2016.07.006
Carvalho, S.A., Palmeira, L., Coutinho, M. et al. (2021). Self-as-context and depressive symptoms in the general population: A further analysis of the self experiences questionnaire. Current Psychology. https://doi.org/10.1007/s12144-021-01383-6
SEQ-8: Yu, L., Scott, W., Goodman, R., Driscoll, L., & McCracken, L. M. (2021). Measuring ‘self’: preliminary validation of a short form of the Self Experiences Questionnaire in people with chronic pain. British Journal of Pain. https://doi.org/10.1177/2049463721994863
SEQ - Polish
SEQ - PolishBaran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
See attachments for female and male versions of the SEQ.
SEQ - Portuguese
SEQ - PortugueseCarvalho, S. A., Palmeira, L., Coutinho, M., Barbosa, R., & Trindade, I. A. (2021). Self-as-context and depressive symptoms in the general population: A further analysis of the Self Experiences Questionnaire. Current Psychology. http://doi.org/10.1007/s12144-021-01383-6
Self-as-Context Scale (SACS)
Self-as-Context Scale (SACS)Zettle, R.D., Gird, S.R., Webster, B.K., Carrasquillo-Richardson, N., Swails, J.A. & Burdsal, C.A. (2018) The Self-as-Context Scale: Development and preliminary psychometric properties. Journal of Contextual Behavioral Science, 10, 64-74. https://doi.org/10.1016/j.jcbs.2018.08.010 The Self-as-Context Scale (SACS) items are in Table 2.
SACS - Chinese
SACS - ChineseFang, S., Huang, M. & Wang, Y. (2022). Measuring self-as-context in Chinese college students: Validity and reliability of the Chinese version of self-as-context scale (C-SACS). Frontiers in Psychology, 13,1051661. DOI: 10.3389/fpsyg.2022.1051661
State measure of experiential avoidance
State measure of experiential avoidancePublished in Kashdan, T. B., Goodman, F. R., Machell, K. A., Kleiman, E. M., Monfort, S. S., & Ciarrochi, J., Nezlek, J. (2014). A contextual approach to experiential avoidance and social anxiety: Evidence from an experimental interaction and daily interactions of people with social anxiety disorder. Emotion.
Survey of Guiding Principles (SGP)
Survey of Guiding Principles (SGP)The Survey of Guiding principles and supporting materials can be downloaded here (they are a bit large for this site):
http://josephciarrochi.com/sgp/
The Survey of Guiding Principles (SGP) was designed to support ACT and also the behavioural components of Cognitive Behavioral Therapy. It helps practitioners to activate value-congruent behavior in their clients.
You can find many materials at http://josephciarrochi.com/sgp/, including:
A manual and guide for using the paper and pencil version of the SGP
A card sort version of the SGP
Printable cards
Sample rating forms for using the SGP card sort in organizations and other settings
References:
- Williams, K., Ciarrochi, J., & Heaven, P. (2015). Relationships between valued action and well-being across the transition from high school to early adulthood. Journal of Positive Psychology, 10, 127-140.
- Veage, S., Ciarrochi, J., & Heaven, P. (2014). Value congruence, importance and success in the workplace: Links with well-being and burnout amongst mental health practitioners. Journal of Contextual Behavioral Science, 3(4), 258-264. https://doi.org/10.1016/j.jcbs.2014.06.004
- Veage, S., Ciarrochi, J., & Heaven, P.C.L. (2011). Importance, Pressure, and Success: Dimensions of Values and their Links to Personality. Personality and Individual Differences, 50, 1180-1185.
Valued Action and Satisfaction Questionnaire (VASQ)
Valued Action and Satisfaction Questionnaire (VASQ)The VASQ is an evolution of the Valued LIving Questionnaire and the Valued Time and Difficulty Questionnaire. Each of these measures assess values with respect to 10-12 life domains (e.g., family, spirituality, etc.). The VASQ contains three subscales: Importance (of values domains), Action (committed action), and Satisfaction (with Action). Each subscale may range from 0-100.
The measure is attached below.
References:
Lyons, G., Stone, B. M., Primeaux, S., Wang, V., & Drake, C. E. (2023). The Valued Action and Satisfaction Questionnaire: Preliminary validation and psychometric evaluation. The Psychological Record. https://doi.org/10.1007/s40732-023-00548-y
Valued Living Scale (VLS)
Valued Living Scale (VLS)References:
Jensen, M.P., Vowles, K.E., Johnson, L.E., & Gertz, K.J. (2015). Living Well with Pain: Development and Preliminary Evaluation of the Valued Living Scale. Pain Medicine, 16(11), 2109–2120. https://doi.org/10.1111/pme.12802 The Valued Living Scale is in the Appendix.
Reilly, E. D., Ritzert, T. R., Scoglio, A. A. J., Mote, J., Fukuda, S. D., Ahern, M. E., & Kelly, M. M. (2019). A systematic review of values measures in acceptance and commitment therapy research. Journal of Contextual Behavioral Science, 12, 290-304. https://doi.org/10.1016/j.jcbs.2018.10.004
Values Tracker (VT)
Values Tracker (VT)Pielech, M., Bailey, R.W., McEntee, M.L., Ashworth, J., Levell, J., Sowden, G., & Vowles, K.E. (2016). Preliminary Evaluation of the Values Tracker: A Two-Item Measure of Engagement in Valued Activities in Those With Chronic Pain. Behavior Modification, 40(1-2) 239–256. DOI: 10.1177/0145445515616911
Vowles, K.E., Sowden, G., Hickman, J., & Ashworth, J. (2019). An analysis of within-treatment change trajectories in valued activity in relation to treatment outcomes following interdisciplinary Acceptance and Commitment Therapy for adults with chronic pain. Behaviour Research and Therapy, 115, 46-54. DOI: 10.1016/j.brat.2018.10.012
Values Wheel
Values WheelBarrett, K., O'Connor, M. & McHugh, L. (2020). Investigating the psychometric properties of the Values Wheel with a clinical cohort: A preliminary validation study. Journal of Contextual Behavioral Science, 15, 210-218. https://doi.org/10.1016/j.jcbs.2019.12.009 The Instructions for the Administration and Completion of the Values Wheel are in Appendix A.
O’Connor, M., Stapleton, A., Barrett, K., Byrne, O., McGinley, N., Slingerland, N., Lee, N., Michalek, S. & McHugh, L.A. (2021). Testing the Psychometric Properties of the Newly Developed ACTive Values Wheel. The Psychological Record, 71, 461–471. https://doi.org/10.1007/s40732-020-00447-6
O’Connor, M., Tennyson, A., Timmons, M. & McHugh, L. (2019). The development and preliminary psychometric properties of the Values Wheel. Journal of Contextual Behavioral Science, 12, 39-46. https://doi.org/10.1016/j.jcbs.2019.01.005
White Bear Suppression Inventory (WBSI)
White Bear Suppression Inventory (WBSI)"Authors: Daniel M. Wegner & Sophia Zanakos
The WBSI is a 15-item questionnaire that is designed to measure thought suppression. Chronic thoughts suppression is a variable that is related to obsessive thinking and negative affect associated with depression and anxiety. The WBSI can help to identify individuals who are more prone to develop chronic thought suppression as well as individuals who express wishing they were not depressed, but are in fact depressed. The measure can also be used by practitioners to evaluate changer over time.
Scoring: The scoring of the WBSI is based on a 5 point scale from Strongly disagree (1) to Strongly agree (5). The total score is obtained by summing up the responses that are provided by respondents. The total score can range from 15 to 75. Higher scores on the WBSI indicate greater tendencies to suppress thoughts.
Reliability: The WBSI has very good internal consistency, with alphas ranging from .87 to .89. The WBSI has also been found to have good stability with a 1 week test-retest correlation of .92, and a 3 week to 3 month test-retest correlation of .69.
Validity: Demonstrates excellent convergent validity with significant correlations between the WBSI and several measures including Beck’s Depression Inventory (BDI), the Maudsley Obsessive-Compulsive Inventory, and the State-Trait Anxiety Inventory (STAI). It has also been found that the WBSI correlates negatively with repression, thus suggesting that the WBSI measures a characteristic that is different to traditional concepts of repression.
Reference: Wegner, D. M. & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62, 615-640."
Information quoted from Ciarrochi, J. & Bilich, L. (2006). Process measures of potential relevance to ACT. Unpublished manuscript, University of Wollongong, Australia.
WBSI - Chinese
WBSI - ChineseRodriguez, M. A., Jia, K., & Qian, M.-y. (2012). White Bear Suppression Inventory: Structure, reliability and validity of the Chinese version. Chinese Journal of Clinical Psychology, 20(2), 143–147.
WBSI - Dutch
WBSI - DutchManon J.B. Vincken, Cor Meesters, Iris M. Engelhard, Erik Schouten (2012). Psychometric qualities of the White Bear Suppression Inventory in a Dutch sample of children and adolescents. Personality and Individual Differences, 52(3), 301-305. https://doi.org/10.1016/j.paid.2011.10.023
WBSI - Finnish
WBSI - FinnishLappalainen, P., Keinonen, K., Pakkala, I., Lappalainen, R., & Nikander, R. (2021). The role of thought suppression and psychological inflexibility in older family caregivers’ psychological symptoms and quality of life. Journal of Contextual Behavioral Science, 20, 129-136. https://doi.org/10.1016/j.jcbs.2021.04.005
WBSI - German Version
WBSI - German VersionWBSI - Deutsche Version: https://contextualscience.org/wbsi_deutsche_version
WBSI - Hungarian
WBSI - HungarianAndrás, H. (2012) KOGNITÍV SÉRÜLÉS ÉS TÜNETI MINTÁZAT KÉNYSZERBETEGSÉGBEN. Budapesti Műszaki és Gazdaságtudományi Egyetem, Dissertation. The WBSI Hungarian translation is in Figure 3.
WBSI - Japanese
WBSI - Japanese(2006) 日本語版 White Bear Suppression Inventory 作成の試み. The Proceedings of the Annual Convention of the Japanese Psychological Association, Volume 70, The 70th Annual Convention of the Japanese Psychological Association, Session ID 2EV114, Pages 2EV114. https://doi.org/10.4992/pacjpa.70.0_2EV114
WBSI - Polish
WBSI - PolishReferences:
1. Baran L., Hyla M., Kleszcz B. (2019). Elastyczność psychologiczna. Polska adaptacja narzędzi dla praktyków i badaczy. Wydawnictwo Uniwersytetu Śląskiego. Read the book online at www.wydawnictwo.us.edu.pl/node/21733
See attachments for male and female versions of the WBSI.
2. Cichoń, E., Szczepanowski, R., & Niemiec, T. (2020). Polish version of the White Bear Suppression Inventory (WBSI) by Wegner and Zanakos: factor analysis and reliability. Skala tłumienia myśli – polska wersja kwestionariusza WBSI (White Bear Suppression Inventory) Wegnera i Zanakos: analiza czynnikowa i rzetelność skali. Psychiatria polska, 54(1), 125–135. https://doi.org/10.12740/PP/93493
WBSI - Spanish Validation
WBSI - Spanish ValidationFernandez-Berrocal, P., Extremera, N., & Ramos, N. (2004). Validity and reliability of the Spanish version of the White Bear Suppression Inventory. Psychological reports, 94(3 Pt 1), 782–784. https://doi.org/10.2466/pr0.94.3.782-784
WBSI - Swedish
WBSI - SwedishSylvan, A., & Lindell, J. (2020). Kom ihåg att glömma: Adaptiv glömska, oro, ruminering & påträngande tankar. Örebro University, Dissertation. The WBSI Swedish translation is in the Appendix (Bilaga A: Översättning av White Bear Suppression Inventory). Retrieved from: https://www.diva-portal.org/smash/record.jsf?pid=diva2%3A1529023&dswid=-328
WBSI Italian
WBSI ItalianWhite Bear Suppression Inventory (WBSI)
Wegner, D. M. & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62, 615-640."
Versione Italiana (1.0) a cura di Lijoi, E., Violini, P., Rossi, E., Melchiorri, E., Ristè, N., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Ristè, N., Violini, P., Melchiorri, E., Lijoi, E.,Rossi, E., Panzera, A., (2014). Italian version of the White Bear Suppression Inventory (WBSI): A preliminary study. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014
Per informazioni: segreteria@aiscc.it – www.aiscc.it
WBSI in Portuguese
WBSI in PortugueseTalask, G. et.al (2018). White Bear Suppression Inventory: translation and cross-cultural adaptation to Brazilian Portuguese. Trends in Psychiatry and Psychotherapy, 40(1). https://doi.org/10.1590/2237-6089-2017-0082
WBSI in Serbian
WBSI in SerbianZdenka Novović, et al (2014) WHITE BEAR SUPPRESSION INVENTORY: VALIDATION OF A SERBIAN TRANSLATION. Primenjena psihologija, Vol 7 No 3-1. https://doi.org/10.19090/pp.2014.3-1.325-345
WBSI in Turkish
WBSI in TurkishYücel Ağargün, M., Beşiroğlu, L., Kemal Kiran, U., Kara, H., & Akil Ozer, O. (2004). Beyaz Ayi Supresyon Envanteri'nin Geçerlik ve Güvenilirliğine Ilişkin Bir On Calişma [The reliability and validity of the White Bear Suppression Inventory]. Turk psikiyatri dergisi, 15(4), 282–290. http://www.turkpsikiyatri.com/default.aspx?modul=ingilizceOzet&gFPrkMakale=484
Translation is at the end of the article.
Willingness and Action Measure for Children and Adolescents (WAM-C/A)
Willingness and Action Measure for Children and Adolescents (WAM-C/A)Greco, L. A., Murrell, A. R., & Coyne, L. W. (2004). The Willingness and Action Measure for Children and Adolescents.
Lidia Cobos-Sánchez, Juan M. Flujas-Contreras, Inmaculada Gómez (2020) Willingness and Action Measure for Adolescents: Psychometric validation in Spanish adolescents. Journal of Contextual Behavioral Science, 15, 46-51. https://doi.org/10.1016/j.jcbs.2019.11.006 The Spanish Version of the WAM-C/A in adolescents is in Appendix A.
WAM-C/A - Spanish
WAM-C/A - SpanishLidia Cobos-Sánchez, Juan M. Flujas-Contreras, Inmaculada Gómez (2020) Willingness and Action Measure for Adolescents: Psychometric validation in Spanish adolescents. Journal of Contextual Behavioral Science, 15, 46-51. https://doi.org/10.1016/j.jcbs.2019.11.006 The Spanish Version of the WAM-C/A in adolescents is in Appendix A.
Compassion Measures
Compassion Measures CommunityCompassionate Engagement and Action Scale (CEAS)
Compassionate Engagement and Action Scale (CEAS)Gilbert, P., Catarino, F., Duarte, C. et al. (2017) The development of compassionate engagement and action scales for self and others. Journal of Compassionate Health Care, 4, 4. https://doi.org/10.1186/s40639-017-0033-3
The CEAS is available on www.compassionatemind.co.uk.
CEAS - Dutch
CEAS - DutchKleissen, Y. (2016) Further validation of The Compassionate Engagement and Action Scales. https://essay.utwente.nl/71044/1/Kleissen_MA_BMS.pdf
CEAS - Japanese
CEAS - JapaneseAsano, K., Kotera, Y., Tsuchiya, M., Ishimura, I., Lin, S., Matsumoto, Y., Matos, M., Basran, J., & Gilbert, P. (2020). The development of the Japanese version of the compassionate engagement and action scales. PloS one, 15(4), e0230875. https://doi.org/10.1371/journal.pone.0230875
CEAS - Slovak
CEAS - SlovakHalamová, J. Kanovský, M., & Pacúchová, M. (2020) PSYCHOMETRIC ANALYSIS OF THE SLOVAK VERSION OF THE COMPASSIONATE ENGAGEMENT AND ACTION SCALES. JPER, 28(1), 64-80.
CEAS - Swedish
CEAS - SwedishHenje, E., Rindestig, F. C., Gilbert, P., & Dennhag, I. (2020). Psychometric validity of the Compassionate Engagement and Action Scale for Adolescents: a Swedish version. Scandinavian journal of child and adolescent psychiatry and psychology, 8, 70–80. https://doi.org/10.21307/sjcapp-2020-007
CEAS - Turkish
CEAS - TurkishAri, E., Cesur-Soysal, G., Basran, J., & Gilbert, P. (2022). The Compassionate Engagement and Action Scales for Self and Others: Turkish Adaptation, Validity, and Reliability Study. Frontiers in Psychology, 13. DOI:10.3389/fpsyg.2022.780077 https://contextualscience.org/compassionate_engagement_and_action_scale_ceas
Self-Compassion Scale (SCS)
Self-Compassion Scale (SCS)Reference: Neff, K. D. (2003). Development and validation of a scale to measure self-compassion. Self and Identity, 2, 223-250. Coding Key: Self-Kindness Items: 5, 12, 19, 23, 26 Self-Judgment Items: 1, 8, 11, 16, 21 Common Humanity Items: 3, 7, 10, 15 Isolation Items: 4, 13, 18, 25 Mindfulness Items: 9, 14, 17, 22 Over-identified Items: 2, 6, 20, 24 Subscale scores are computed by calculating the mean of subscale item responses. To compute a total self-compassion score, reverse score the negative subscale items - self-judgment, isolation, and over-identification - then compute a total mean. (This method of calculating the total score is slightly different than that used in the article referenced above, in which each subscale was added together. However, I find it is easier to interpret the scores if the total mean is used.)
SCS - Arabic
SCS - ArabicHawa Alabdulaziz, Nahed Alquwez, Joseph U. Almazan, Abdulrhman Albougami, Farhan Alshammari, Jonas Preposi Cruz (2020). The Self-Compassion Scale Arabic version for baccalaureate nursing students: A validation study. Nurse Education Today, 89.
https://doi.org/10.1016/j.nedt.2020.104420
SCS - Chinese
SCS - ChineseChen J, Yan L & Zhou L. (2011). Reliability and validity of Chinese version of Self-compassion Scale. Chinese Journal Of Clinical Psychology, 19(6), 734-736.
The Chinese SCS translation is on www.self-compassion.org.
SCS - Czech
SCS - CzechBenda, J., & Reichová, A. (2016). Psychometrické charakteristiky české verze Self-Compassion Scale (SCS-CZ). Československá psychologie, 60(2), 120-136.
Benda, J. (2018). Alternative models of the Czech version of the Self-Compassion Scale (SCS-26-CZ). http://doi.org/ 10.13140/RG.2.2.26763.18724
The Czech SCS translation is on www.self-compassion.org.
SCS - Estonian
SCS - EstonianTeri Talpsep (2015) MEASURING MINDFULNESS AND SELF-COMPASSION: A QUESTIONNAIRE AND ERP STUDY. Master’s Thesis, University of Tartu. The Estonian version of the self compassion scale (SCS) is in the Appendix.
SCS - French
SCS - FrenchKotsou I, Leys C (2016) Self-Compassion Scale (SCS): Psychometric Properties of The French Translation and Its Relations with Psychological Well-Being, Affect and Depression. PLoS ONE.
The SCS French translation is on www.self-compassion.org
SCS - German
SCS - GermanHupfeld, J. & Ruffieux, N. (2011). Validierung einer deutschen Version der Self-Compassion Scale (SCS-D). Zeitschrift für Klinische Psychologie und Psychotherapie, 40 (2), 115–123.
The SCS German translation is on www.self-compassion.org.
SCS - Greek
SCS - GreekKarakasidou, E., Pezirkianidis, C., Galanakis, M., & Stalikas, A. (2017). Validity, Reliability and Factorial Structure of the Self Compassion Scale in the Greek Population. Journal of Psychology & Psychotherapy, 7, 313. DOI: 10.4172/2161-0487.1000313
Αλαθνξά: Mantzios, M., Wilson, J. C., & Giannou, K. (2015). Psychometric Properties of the Greek Versions of the Self-Compassion and Mindful Attention and Awareness Scales. Mindfulness, 6(1), 123-132.
The SCS Greek Translation is on www.self-compassion.org.
SCS - Hungarian
SCS - HungarianTóth-Király, I., Bőthe, B. & Orosz, G. (2017) Exploratory Structural Equation Modeling Analysis of the Self-Compassion Scale. Mindfulness, 8, 881–892. https://doi.org/10.1007/s12671-016-0662-1
Sági, Andrea & Köteles, Ferenc & V.Komlósi, Annamária. (2013). Az Önmagunk Iránt Érzett Együttérzés (Önegyüttérzés) skála magyar változatának pszichometriai jellemzői [Psychometric characteristics of the Hungarian version of the Self-Compassion (Self-Compassion) scale]. Pszichológia, 33, 293-312. http://doi.org/10.1556/Pszicho.33.2013.4.3.
The SCS Hungarian translation is on www.self-compassion.org.
SCS - Icelandic
SCS - IcelandicSigurðardóttir, A.A. (2020). The Role of Self-Compassion in Music Performance Anxiety. Thesis. Reykjavík University, Reykjavík, Iceland. Retrived from https://skemman.is/handle/1946/36443 The Self-Compassion Scale Icelandic Version is in Appendix D.
Gunnarsdóttir, Á. S. (2019). Correlation of self-compassion, BMI, depression, anxiety, stress and gender in individuals seeking obesity treatment and university students. Thesis. Reykjavík University, Reykjavík, Iceland. Retrieved from http://hdl.handle.net/1946/32924
SCS - Indonesian
SCS - IndonesianSugianto, D., Suwartono, C., & Sutanto, S. H. (2020). Reliabilitas dan validitas SelfCompassion Scale versi bahasa Indonesia. Jurnal Psikologi Ulayat. http://doi.org/10.24854/jpu02020-337
The SCS Indonesian translation is on www.self-compassion.org.
SCS - Italian
SCS - ItalianSelf Compassion Scale (SCS)
Neff, K.D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223-250. DOI: 10.1080/15298860390209035
Referenza bibliografica: Rossi, E., Melchiorri, E., Panzera., A., Romitelli M. (2015). A preliminary study on validating the Self-Compassion Scale (SCS) in Italian adolescents. Poster presented at ACBS World Conference 13 Poster Session – Berlin, German- July 14-19, 2015. Il presente studio è in corso di aggiornamento. Per informazioni: segreteria@aiscc.it – www.aiscc.it
Veneziani, C. A., Fuochi, G., & Voci, A. (2017). Self-compassion as a healthy attitude toward the self: Factorial and construct validity in an Italian sample. Personality and Individual Differences, 119, 60-68. doi:10.1016/j.paid.2017.06.028 Contatto: alberto.voci@unipd.it
The SCS Italian translation is on www.self-compassion.org
SCS - Japanese
SCS - JapaneseArimitsu, K. (2014). Development and validation of the Japanese version of the Self-Compassion Scale. Japanese Journal of Psychology, 85(1), 50-59. The SCS Japanese translation is on www.self-compassion.org
SCS - Korean
SCS - KoreanLee, W. K., & Lee, K. (2010). The Validation Study of the Korean Version of Self-Compassion Scale with Adult Women in Community. Journal of Korean Neuropsychiatric Association, 49(2), 193–200.
The SCS Korean translation is on www.self-compassion.org.
SCS - Lithuanian
SCS - LithuanianDiržytė, Aistė & Sabaitytė, Eglė (2016) Psychological capital, self-compassion, and life satisfaction of unemployed youth. International Journal of Psychology: Biopsychosocial Approach 2016 / 19. http://doi.org/10.7220/2345-024X.19.3
SCS - Malay
SCS - MalayAbd Hamid, H. S., Saleh, B. S., Azmi, F., Doan, H. T., Lee, X. J., Lim, J. Y, Che Sakari, N. S., Ooi, G. S., & Jie., Y. S. (2019). VALIDATION OF THE SELF-COMPASSION SCALE IN A MALAYSIAN SAMPLE. International Journal of Education, Psychology and Counseling, 4 (25). 22-32. http://www.ijepc.com/PDF/IJEPC-2019-25-03-02.pdf
SCS - Norwegian
SCS - NorwegianDundas, I., Svendsen, J. L., Wiker, A. S., Granli, K. V., & Schanche, E. (2016). Selfcompassion and depressive symptoms in a Norwegian student sample. Nordic Psychology, 68(1), 58-72. http://dx.doi.org/10.1080/19012276.2015.1071203
(se «Supplementary Material» til denne artikkelen for de psykometriske egenskapene til norsk versjon av SCS)
The SCS Norwegian translation is on www.self-compassion.org.
SCS - Persian/Farsi
SCS - Persian/FarsiMOMENI, F., & SHAHIDI, S., & MOOTABI, F., & HEYDARI, M. (2014). PSYCHOMETRIC PROPERTIES OF A FARSI VERSION OF THE SELF-COMPASSION SCALE (SCS). CONTEMPORARY PSYCHOLOGY, 8(2 (16)), 27-40. https://www.sid.ir/en/journal/ViewPaper.aspx?id=376431
The Self-Compassion Scale Persian translation is on www.self-compassion.org.
SCS - Portuguese
SCS - PortugueseSouza, L. K. de, & Hutz, C. S. (2016). Escala de Autocompaixão. In C. S. Hutz (Ed.), Avaliação em Psicologia Positiva (171-173). São Paulo: CETEPP.
Castilho, P., Pinto-Gouveia, J., & Duarte, J., (2015). Evaluating the Multifactor Structure of the Long and Short Versions of the Self-Compassion Scale in a Clinical Sample. Journal of Clinical Psychology. http://doi.org/10.1002/jclp.22187
The Brazilian Portuguese SCS translation is on www.self-compassion.org.
The Portuguese SCS translation is on www.self-compassion.org.
SCS - Russian
SCS - RussianЧистопольская К.А., Осин Е.Н., Ениколопов С.Н., Николаев Е.Л., Мысина Г.А., Дровосеков С.Э. (2020) Концепт «Сочувствие к себе»: российская адаптация опросника Кристин Нефф. [The Сoncept of Self-compassion: a Russian Adaptation of the Scale by Kristin Neff] Культурно-историческая психология, 16(4), 35–48. http://doi.org/10.17759/chp.2020160404 The Self Compassion Scale Russian translation is in the article.
SCS - Serbian
SCS - SerbianThe Self-Compassion Scale (SCS) Serbian Translation can be found on the Repository of psychological instruments in Serbian [Repozitorijum psiholoških instrumenata na srpskom jeziku] (REPOPSI). https://doi.org/10.17605/OSF.IO/5ZB8P
SCS - Sinhala
SCS - Sinhalade Zoysa, P., Kumar, S., Amarasuriya, S.D. & Mendis, N.S.R. (2021). Cultural validation of the Self-Compassion Scale and the Subjective Happiness Scale and the influence of gender on self-compassion and subjective happiness in a Sri Lankan undergraduate population. Asian Journal of Social Psychology. https://doi.org/10.1111/ajsp.12505
SCS - Slovak
SCS - SlovakHalamová, J., Kanovský, M., & Pacúchová, M. (2018). Self-Compassion Scale: IRT Psychometric Analysis, Validation, and Factor Structure - Slovak Translation. Psychologica Belgica, 57(4), 190–209. https://doi.org/10.5334/pb.398 Slovak translation is in Appendix 1.
Halamová, J., Kanovský, M., & Pacúchová, M. (2018). Self-Compassion Scale--Slovak Version (SCS). APA PsycTests. https://doi.org/10.1037/t68832-000
The SCS Slovak Transation is on www.self-compassion.org.
SCS - Slovenian
SCS - SlovenianNika Uršič, Daša Kocjančič, Gregor Žvelc (2019) Psychometric Properties of the Slovenian Long and Short Version of the Self-Compassion Scale. Psihologija, 52(2), 107-125. https://doi.org/10.2298/PSI180408029U
The SCS Slovenian translation is on www.self-compassion.org.
SCS - Spanish
SCS - SpanishGarcia-Campayo J, Navarro-Gil M, Andrés E, Montero-Marin J, López-Artal L, Demarzo MM. (2014). Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the SelfCompassion Scale (SCS). Health Qual Life Outcomes, 12(4). http://doi.org/10.1186/1477-7525-12-4
The SCS Spanish translation is on www.self-compassion.org
SCS - Thai
SCS - ThaiKatsumata, M. & Mohanan, S.A. (2020) The Influence of Self-Concept on Resilience Being Mediated by Self-Compassion and Compassion for Others Among Thai Adolescents. Scholar : Human Sciences, 12(1), 20-36.
SCS - Turkish
SCS - TurkishDeniz, M. E., Kesici Ş., & Sümer, A. S. (2008). The validity and reliability study of the Turkish version of self-compassion scale. Social Behavior and Personality, 36 (9), 1151-1160.
The SCS Turkish translation is on www.self-compassion.org.
SCS - Ukrainian
SCS - UkrainianСахнюк Роксолана Володимирівна (2021). Психометричні властивості української версії Фрайбурзького опитувальника майндфулнес на вибірці повнолітнього. Магістерська робота, Український католицький університет. [Sakhniuk R.V. (2021). Psychometric properties of the Ukrainian version of Freiburg Mindfulness questionnaire on a sample of adults. Master's thesis, Ukrainian Catholic University.] The Self-Compassion Scale (SCS) Ukrainian version is in the appendix. http://www.er.ucu.edu.ua/bitstream/handle/1/2763/Sakhniuk_mag.pdf
SCS - Urdu
SCS - UrduBibi, S. et al. (2017) Effect of Self-Compassion on the Marital Adjustment of Pakistani Adults. Foundation University Journal of Psychology, 1(2), 52-66. https://fui.edu.pk/fjs/index.php/fujp/article/view/52
SCS - Vietnamese
SCS - VietnameseNguyen Phuoc, C. & Ngoc Nguye, Q-A. (2020). Self-Compassion and Well-being among Vietnamese Adolescents. International Journal of Psychology & Psychological Therapy, 20 (3), 327-341.
Self-Compassion Scale - Short Form (SCS-SF)
Self-Compassion Scale - Short Form (SCS-SF)Raes, F., Pommier, E., Neff, K.D. & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology and Psychotherapy, 18, 250-255. https://doi.org/10.1002/cpp.702
The SCS-SF is on self-compassion.org.
SCS-SF - Chinese
SCS-SF - ChineseMeng, R., Yu, Y., Chai, S., Luo, X., Gong, B., Liu, B., Hu, Y., Luo, Y., & Yu, C. (2019). Examining psychometric properties and measurement invariance of a Chinese version of the Self-Compassion Scale - Short Form (SCS-SF) in nursing students and medical workers. Psychology research and behavior management, 12, 793–809. https://doi.org/10.2147/PRBM.S216411
SCS-SF - Dutch
SCS-SF - DutchRaes F, Pommier E, Neff KD, Van Gucht D. (2011) Construction and factorial validation of a short form of the Self-Compassion Scale. Clin Psychol Psychother, 18(3), 250-5. http://doi.org/10.1002/cpp.702
The Dutch SCS-Short Form translation is on www.self-compassion.org.
SCS-SF - Italian
SCS-SF - ItalianVeneziani, Chiara A. (2015) Consapevolezza, accettazione e comprensione di sé: associazioni con il benessere individuale e l'apertura prosociale. [Dissertation]. The Italian Self-Compassion Scale Short Form items are in Tabella 2.1.
SCS-SF - Japanese
SCS-SF - JapaneseMihoko NAKAMINE,Munenaga KODA,Yoshinori ITO and Hiroshi SATO (2015) Self-Compassion Scale Short Form 中学生版の作成と 信頼性・妥当性の検討 [Development of the Self-Compassion Scale Short Form for Junior High School Students]. 関西大学『社会学部紀要』第47巻第 1 号,2015,21‒30. The Japanese SCS-SF items are in table 1.
SCS-SF - Persian
SCS-SF - PersianKhanjani S, Foroughi A A, Sadghi K, Bahrainian S A. (2016) Psychometric properties of Iranian version of self-compassion scale (short form) . Pajoohande, 21(5), 282-289.
URL: http://pajoohande.sbmu.ac.ir/article-1-2292-en.html
SCS-SF - Portuguese
SCS-SF - PortugueseReferences:
Rocha, L., Braga Pereira, L., & Leonel Peluso, M. (2022). Self-Compassion Scale - Short Form (SCS-SF): initial evidence of validity in Brazil. Revista Psicologia em Pesquisa, 16(2).
Castilho, P., Pinto-Gouveia, J., & Duarte, J., (2015). Evaluating the Multifactor Structure of the Long and Short Versions of the Self-Compassion Scale in a Clinical Sample. Journal of Clinical Psychology, 71, 856-870. http://doi.org/10.1002/jclp.22187
SCS-SF - Slovenian
SCS-SF - SlovenianNika Uršič, Daša Kocjančič, Gregor Žvelc (2019) Psychometric Properties of the Slovenian Long and Short Version of the Self-Compassion Scale. Psihologija, 52(2), 107-125. https://doi.org/10.2298/PSI180408029U
SCS-SF - Spanish
SCS-SF - SpanishReferences
Lluch-Sanz, C., Galiana, L., Vidal-Blanco, G., & Sansó, N. (2022) Psychometric Properties of the Self-Compassion Scale—Short Form: Study of Its Role as a Protector of Spanish Nurses Professional Quality of Life and Well-Being during the COVID-19 Pandemic. Nursing Reports, 12, 65-76. https://doi.org/10.3390/nursrep12010008
Garcia-Campayo J, Navarro-Gil M, Andrés E, Montero-Marin J, López-Artal L, Demarzo MM. (2014). Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the SelfCompassion Scale (SCS). Health Qual Life Outcomes, 12(4). http://doi.org/10.1186/1477-7525-12-4 The SCS-SF Spanish version is in the Annex.
SCS-SF - Swedish
SCS-SF - SwedishAnna Bratt & Cecilia Fagerström (2020) Self-compassion in old age: confirmatory factor analysis of the 6-factor model and the internal consistency of the Self-compassion scale-short form. Aging & Mental Health, 24(4), 642-648. http://doi.org/10.1080/13607863.2019.1569588
Self-Compassion Scale for Youth (SCS-Y)
Self-Compassion Scale for Youth (SCS-Y)Kristin D. Neff, Karen Bluth, István Tóth-Király, Oliver Davidson, Marissa C. Knox, Zachary Williamson & Andrew Costigan (2021) Development and Validation of the Self-Compassion Scale for Youth. Journal of Personality Assessment, 103, 1, 92-105. DOI: 10.1080/00223891.2020.1729774
The SCS-Y is available on self-compassion.org.
SCS-A - Portuguese
SCS-A - PortugueseCunha, M., Xavier, A., & Vitória, I. (2013). Avaliação da auto-compaixão em adolescentes: Adaptação e qualidades psicométricas da Escala de Auto-Compaixão. [Assessment of self-compassion in adolescents: Adaptation and psychometric properties of the Self-Compassion Scale]. Revista de Psicologia da Criança e do Adolescente [Journal of Child and Adolescent Psychology], 4(2), 95-117. Retrieved from https://estudogeral.uc.pt/bitstream/10316/46877/1/2013_Avalia%c3%a7%c3%a3o%20da%20auto-compaix%c3%a3o%20em%20adolescentes.pdf
SCS-CA - German
SCS-CA - GermanGruber, E., Baumann, I., Vonderlin, E. et al. (2023). Translation and Factorial Validation of the Self-Compassion Scale for Adolescents in a German Community Sample. Journal of Child and Family Studies, 32, 1318–1331. https://doi.org/10.1007/s10826-023-02569-1
SCS-Y - Greek
SCS-Y - GreekKarakasidou, E. , Raftopoulou, G. , Pezirkianidis, C. & Stalikas, A. (2021). Validity, Reliability and Factorial Structure of the Self Compassion Scale-Youth Version in the Greek Population. Psychology, 12, 536-553. http://doi.org/10.4236/psych.2021.124033.
SCS-Y - Persian
SCS-Y - PersianNazari, N., Hernández, R.M., Ocaña-Fernandez, Y. et al. (2022). Psychometric Validation of the Persian Self-Compassion Scale Youth Version. Mindfulness, 13, 385–397. https://doi.org/10.1007/s12671-021-01801-7
SCS-Y - Thai
SCS-Y - ThaiSelf-Compassion Scale for Youth-Thai version is available on https://self-compassion.org/
SCS-Y - Turkish
SCS-Y - TurkishÇAKMAK, Aygen; KANAK, Mehmet; ÖZKUBAT, Seda (2018). ÇOCUKLAR İÇİN ÖZ ŞEFKAT ÖLÇEĞİ: TÜRKÇEYE UYARLAMA ÇALIŞMASI. [SELF-COMPASSION SCALE FOR CHILDREN: TURKISH ADAPTATION STUDY.] Electronic Turkish Studies, 13(26), 295-305.
State Self Compassion Scale
State Self Compassion ScaleFor an experimental study on perspective taking on self relevant negtaive thoughts, we adapted the self compassion scale short form to be a state version. The manuscript is under review, here is how we decirbed the measure:
2.4.3. State Self-Compassion Scale (SSCS)
The SSCS is an adapted seven item, self-report measure based on the 26 item Self- Compassion Scale (SCS; Neff, 2003b). The SCS contains six subscales: Self-Kindness, Self- Judgement, Common Humanity, Isolation, Mindfulness and Over-Identification. The original SCS demonstrated good discriminant validity, test-retest reliability (r = .93) and internal reliability (Cronbach's α = .92). The adapted version for the present study included one item from each subscale and an additional item from the Self-Kindness subscale. The wording was also modified to measure state rather than trait self-compassion for a specific thought. Example items include, “As I think this thought right now, I am being disapproving and judgmental towards myself,” and “As I have this thought right now, I am able to be understanding and patient towards those aspects of myself that I don't like”. The resulting scale for this study was the State Self-Compassion Questionnaire, consisting of 7 items measured on a 5-point Likert scale, with possible answers ranging from ‘almost never’ to ‘almost always’. In the present study, the SSCS demonstrated good internal reliability (α = .73). Likewise, Pendrous and Hulbert-Williams (2017) developed a similar state adaptation of the SCS that had a reported alpha of .78.
To make the measure more generally useable in experimental preparations the version attahced her has had the words 'As I think this thought' removed. Items, scoring details and brief psychometric properties are in the attached document.
**** Whilst preparing this I found that Kristin Neff has actually published a state version of the Self Compassion Scale Short Form, in Septmber 2020. It wasn't available when we were looking for such a measure****
You can access that published version here and the article describing it here. It has much better validation that the quick adaptation we made, so I would reccomedn using that scale instead.
The citation for that scale is: Neff, K. D., Tóth-Király, I., Knox, M., Kuchar, A. & Davidson, O. (2020). The development and validation of the State Self-Compassion Scale (long and short form). Mindfulness. Advance online publication. DOI:10.1007/s12671-020-01505-4
SSCS - Japanese
SSCS - JapaneseChishima, Y., Sugawara, D., & Mizuno, M. (2022, April 26). Supportive Evidence for the State Self-Compassion Scale Using Japanese Samples. https://doi.org/10.1037/pas0001144 The Japanese Version of the State Self-Compassion Scale 日本語版状態セルフ・コンパッション尺度 is in the Appendix.
SSCS - Spanish
SSCS - SpanishThe Escala de Autocompasión-estado (Spanish State Self-Compassion Scale) is available on https://self-compassion.org
FAP Measures
FAP Measures CommunityAwareness, Courage, and Responsiveness Scale (ACRS)
Awareness, Courage, and Responsiveness Scale (ACRS)Kuczynski, A.M. et al (2020) Measuring intimacy as a contextual behavioral process: Psychometric development and evaluation of the Awareness, Courage, and Responsiveness Scale. Journal of Contextual Behavioral Science, 16, 199-208. https://doi.org/10.1016/j.jcbs.2019.02.004 The ACRS items are in Table 2.
ACRS - Spanish
ACRS - SpanishOrtiz-Fune, C., Arias, M.F., Martínez-Cervantes, R.J. (2021) Spanish Adaptation of the Awareness, Courage and Responsiveness Scale: Preliminary Psychometric Properties in Non-clinical Samples. Journal of Contextual Behavioral Science. https://doi.org/10.1016/j.jcbs.2021.06.006 The Spanish translation of the ACRS items are in Table 2.
Experiencing of Self Scale (EOSS)
Experiencing of Self Scale (EOSS)Experiencing of Self Scale (EOSS) for assessment in FAP
Valero-Aguayo, L., Ferro-García, R., López-Bermúdez, M. ángel, & Selva-López De Huralde, M. D. L. ángeles. (2014). Psychometric properties of the Spanish version of the Experiencing Of Self Scale (EOSS) for assessment in functional analytic psychotherapy. Psicothema, 26(3), 415-422. https://reunido.uniovi.es/index.php/PST/article/view/10490 The original EOSS and the translation are in Table 1.
Kanter, J. W., Parker, C. R., & Kohlenberg, R. J. (2001). Finding the self: A behavioral measure and its clinical implications. Psychotherapy: Theory, Research, Practice, Training, 38(2), 198-211.
EOSS - Spanish
EOSS - SpanishValero-Aguayo, L., Ferro-García, R., López-Bermúdez, M. ángel, & Selva-López De Huralde, M. D. L. ángeles. (2014). Psychometric properties of the Spanish version of the Experiencing Of Self Scale (EOSS) for assessment in functional analytic psychotherapy. Psicothema, 26(3), 415-422. The original EOSS and the translation are in Table 1.
Functional Analytic Psychotherapy Intimacy Scale (FAPIS)
Functional Analytic Psychotherapy Intimacy Scale (FAPIS)Leonard, R.C., Knott, L.E., Lee, E.B. et al. (2014). The Development of the Functional Analytic Psychotherapy Intimacy Scale. The Psychological Record, 64, 647–657. https://doi.org/10.1007/s40732-014-0089-
Singh, R.S., Wetterneck, C., & O'Brien, W. (2020). Psychometric evaluation of the Functional Analytic Psychotherapy Intimacy Scale in obsessive-compulsive and related disorders. Bulletin of the Menninger Clinic, 84(2), 156-179. https://doi.org/10.1521/bumc_2020_84_06
Functional Idiographic Assessment Template (FIAT)
Functional Idiographic Assessment Template (FIAT)Callaghan, G. M. (2006). The Functional Idiographic Assessment Template (FIAT) system: For use with interpersonally-based interventions including Functional Analytic Psychotherapy (FAP) and FAP-enhanced treatments. The Behavior Analyst Today, 7(3), 357-398. http://dx.doi.org/10.1037/h0100160 The FIAT is in the article.
Functional Idiographic Assessment Template-Questionnaire (FIAT-Q)
Functional Idiographic Assessment Template-Questionnaire (FIAT-Q)Darrow, S.M., Callaghan, G.M., Bonow, J.T., & Follette, W.C. (2014). The Functional Idiographic Assessment Template-Questionnaire (FIAT-Q): Initial psychometric properties. Journal of Contextual Behavioral Science, 3(2), 124-135. https://doi.org/10.1016/j.jcbs.2014.02.002 The FIAT-Q is in the appendix.
FIAT-Q - Polish
FIAT-Q - PolishKwestionariusz dotyczący relacji interpersonalnych autorstwa Glenna M. Callaghana w polskim tłumaczeniu Marcina Domurata i Jana Topczewskiego.
The FIAT-Q Polish translation can be found on the ACBS Poland Chapter website. https://acbs.pl/zasoby/materialy/
Life Snapshot Inventory (LSI)
Life Snapshot Inventory (LSI)Ruiz-García, A., Macías-Morón, J. J., Ferro-García, R., & Valero-Aguayo, L. (2021). Spanish Validation of the "Life Snapshot Inventory". International journal of psychological research, 14(2), 9–17. https://doi.org/10.21500/20112084.5095
Aldahadha B. (2023). Validity of the Jordanian Version of the Life Snapshot Inventory. Social Sciences, 12(2), 57. https://doi.org/10.3390/socsci12020057
LSI - Arabic
LSI - ArabicAldahadha B. (2023). Validity of the Jordanian Version of the Life Snapshot Inventory. Social Sciences, 12(2), 57. https://doi.org/10.3390/socsci12020057
LSI - Spanish
LSI - SpanishRuiz-García, A., Macías-Morón, J. J., Ferro-García, R., & Valero-Aguayo, L. (2021). Spanish Validation of the "Life Snapshot Inventory". International journal of psychological research, 14(2), 9–17. https://doi.org/10.21500/20112084.5095
Miscellaneous Measures
Miscellaneous Measures CommunityRFT Measures
RFT MeasuresRFT Measures of Acceptance and Experiential Avoidance
- Levin, M.E., Haeger, J. & Smith, G.S. Examining the Role of Implicit Emotional Judgments in Social Anxiety and Experiential Avoidance. J Psychopathol Behav Assess 39, 264–278 (2017). https://doi.org/10.1007/s10862-016-9583-5
- Drake, C.E., Timko, C.A. & Luoma, J.B. Exploring an Implicit Measure of Acceptance and Experiential Avoidance of Anxiety. Psychol Rec 66, 463–475 (2016). https://doi.org/10.1007/s40732-016-0186-z
RFT Measures of Clinical Issues
- Chan, G., Dermot Barnes-Holmes, D., Barnes-Holmes, Y. Stewart, I. (2009) Implicit Attitudes to Work and Leisure Among North American and Irish Individuals: A Preliminary Study. International Journal of Psychology and Psychological Therapy, 9(3), 317-334.
- Cullen, C., Barnes-Holmes, D., Barnes-Holmes, Y. et al. The Implicit Relational Assessment Procedure (IRAP ) and the Malleability of Ageist Attitudes. Psychol Rec 59, 591–620 (2009). https://doi.org/10.1007/BF03395683
- Power, P., Barnes-Holmes, D., Barnes-Holmes, Y. et al. The Implicit Relational Assessment Procedure (IRAP) as a Measure of Implicit Relative Preferences: A First Study. Psychol Rec 59, 621–640 (2009). https://doi.org/10.1007/BF03395684
- Vahey, N.A., Barnes-Holmes, D., Barnes-Holmes, Y. et al. A First Test of the Implicit Relational Assessment Procedure as a Measure of Self-Esteem: Irish Prisoner Groups and University Students. Psychol Rec 59, 371–387 (2009). https://doi.org/10.1007/BF03395670
- Dawson, D. L., Barnes-Holmes, D., Gresswell, D. M., Hart, A. J. P., & Gore, N. J. (2009). Assessing the implicit beliefs of sexual offenders using the Implicit Relational Assessment Procedure: A First Study. Sexual Abuse: A Journal of Research and Treatment, 21(1), 57-75.
Shame Measures
Shame Measures CommunityChronic Illness-related Shame Scale (CISS)
Chronic Illness-related Shame Scale (CISS)Trindade, I. A., Ferreira, C., & Pinto-Gouveia, J. (2017). Chronic illness-related shame: Development of a new scale and novel approach for IBD patients’ depressive symptomatology. Clinical Psychology and Psychotherapy, 24(1), 255–263. doi: 10.1002/cpp.2035
(original version in Portuguese from Portugal)
CISS - Portuguese
CISS - PortugueseTrindade, I. A., Ferreira, C., & Pinto-Gouveia, J. (2017). Chronic illness-related shame: Development of a new scale and novel approach for IBD patients’ depressive symptomatology. Clinical Psychology and Psychotherapy, 24(1), 255–263. doi: 10.1002/cpp.2035
(original version in Portuguese from Portugal)
Internalized Shame Scale (ISS)
Internalized Shame Scale (ISS)Internalized Shame Scale. Reference: Rosario, P.M. & White, R.M. (2006). The Internalized Shame Scale: Temporal stability, internal consistency, and principal components analysis. Personality and Individual Differences, 41, 95–103.
ISS - Italian
ISS - ItalianINTERNALIZED SHAME SCALE (ISS)
Rosario, P.M. & White, R.M. (2006). The Internalized Shame Scale: Temporal stability, internal consistency, and principal components analysis. Personality and Individual Differences, 41, 95–103.
Traduzione Italiana (1.0) a cura di Lijoi, E., Cioci, M., Francesconi, C., Rossi, E., Melchiorri, E., Violini, P., Ristè, N. (2013) AISCC, Gruppo Ricerca ACT.
Traduzione Italiana (2.0) a cura di Violini, P., Lijoi, E., Ristè, N., Rossi, E., Melchiorri, E., (2014) AISCC, Gruppo Ricerca ACT.
Referenza bibliografica: Lijoi, E., Violini, P., Rossi, E., Melchiorri, E., Ristè, N., Panzera, A., (2014). Validity and reliability of an Italian version of the Internalized Shame Scale (ISS) for Youth. Poster presented at ACBS World Conference 12 Poster Session - Minneapolis, Minnesota, USA - June 17-22, 2014.
Per informazioni: segreteria@aiscc.it – www.aiscc.it
ISS - Korean
ISS - KoreanInsuk Lee, Haerim Choi. (2005) Validation Study of the Internalized Shame Scale (ISS). Journal of the Korean Psychological Association: Counseling and Psychotherapy, 17.3, 651-670.
ISS - Norwegian
ISS - NorwegianArne Vikan, Anne Marit Hassel, Arild Rugset, Hedda Eline Johansen & Tomas Moen (2010) A test of shame in outpatients with emotional disorder. Nordic Journal of Psychiatry, 64(3), 196-202. DOI: 10.3109/08039480903398177
ISS - Portuguese
ISS - PortugueseMatos, M., Pinto-Gouveia, J., & Duarte, C. (2012). When I don't Like Myself: Portuguese Version of the Internalized Shame Scale. The Spanish Journal of Psychology, 15(3), 1411-1423. http://doi.org/10.5209/rev_SJOP.2012.v15.n3.39425
Stigma Measures
Stigma Measures CommunityPerceived Stigma of Substance Abuse Scale (PSAS)
Perceived Stigma of Substance Abuse Scale (PSAS)Perceived Stigma of Substance Abuse Scale (PSAS) is attached. Login to your ACBS account to see the attachment.
Luoma, J. B., O'Hair, A. K., Kohlenberg, B. S., Hayes, S. C., Fletcher, L. (2010). The development and psychometric properties of a new measure of perceived stigma toward substance users. Substance Use and Misuse, 45, 47-57.
PSAS - Hindi
PSAS - HindiMattoo, S.K. & Sarkar, S. (2012). Validation of Hindi version of perceived stigma of substance abuse scale. Indian Journal of Social Psychiatry, 28 (3-4), 117-120. The full text of the article can be found on researchgate.net.
PSAS - Vietnam
PSAS - VietnamStockton, M. A., Mughal, A. Y., Bui, Q., Greene, M. C., Pence, B. W., Go, V., & Gaynes, B. N. (2021). Psychometric performance of the perceived stigma of substance abuse scale (PSAS) among patients on methadone maintenance therapy in Vietnam. Drug and alcohol dependence, 226, 108831. Advance online publication. https://doi.org/10.1016/j.drugalcdep.2021.108831
Stigmatizing Attitudes–Believability (SAB)
Stigmatizing Attitudes–Believability (SAB)Assesses believability of negative thoughts towards clients.
Reference: Hayes, S. C., Bissett, R., Roget, N., Padilla, M., Kohlenberg, B. S., Fisher, G., Masuda, A., Pistorello, J., Rye, A. K., Berry, K. & Niccolls, R. (2004). The impact of acceptance and commitment training and multicultural training on the stigmatizing attitudes and professional burnout of substance abuse counselors. Behavior Therapy, 35, 821-835.
Substance Abuse Self-Stigma Scale (SASSS)
Substance Abuse Self-Stigma Scale (SASSS)Substance Abuse Self-Stigma Scale (SASSS) is attached. Please login to your ACBS account to see the attachment.
Luoma, J.B.,Nobles, R. H., Drake, C., E., Hayes, S. C., O-Hair, A., Fletcher, L., & Kohlenberg, B. S. (2013). Self-Stigma in Substance Abuse: Development of a New Measure. Journal of Psychopathology and Behavioral Assessment, 34, 1-12.
Weight Self-Stigma Questionnaire (WSSQ)
Weight Self-Stigma Questionnaire (WSSQ)Lillis, J., Luoma, J.B., Levin, M.E., & Hayes, S.C. (2010). Measuring weight self-stigma: The Weight Self-Stigma Questionnaire. Obesity, 18(5), 971-976.
The WSSQ is available at stevenchayes.com.
WSSQ - Arabic
WSSQ - ArabicBinDhim N.F., Althumiri N.A., Basyouni M.H., Sims O.T., Alhusseini N., & Alqahtani S.A. (2020) Arabic Translation of the Weight Self-Stigma Questionnaire: Instrument Validation Study of Factor Structure and Reliability.
JMIR Formative Research, 4(11), e24169. doi: 10.2196/24169 Arabic Translation of the WSSQ is in the Multimedia Appendix 1.
WSSQ - Chinese
WSSQ - ChineseLin, K. P., & Lee, M. L. (2017). Validating a Chinese version of the Weight Self-stigma Questionnaire for use with obese adults. International Journal of Nursing Practice, 23(4). https://doi.org/10.1111/ijn.12537
WSSQ - French
WSSQ - FrenchMaïano, C., Aimé, A., Lepage, G., ASPQ Team, & Morin, A. (2019). Psychometric properties of the Weight Self-Stigma Questionnaire (WSSQ) among a sample of overweight/obese French-speaking adolescents. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity, 24(3), 575–583. https://doi.org/10.1007/s40519-017-0382-0 The French translation of the WSSQ is in table 3.
WSSQ - German
WSSQ - GermanHain, B., Langer, L., Hünnemeyer, K. et al. (2015). Translation and Validation of the German Version of the Weight Self-Stigma Questionnaire (WSSQ). Obesity Surgery. 25, 750–753. https://doi.org/10.1007/s11695-015-1598-6
WSSQ - Italian
WSSQ - ItalianRossi, A.A., Manzoni, G.M., Pietrabissa, G. et al. (2022). Weight stigma in patients with overweight and obesity: validation of the Italian Weight Self-Stigma Questionnaire (WSSQ). Eating and Weight Disorders, 27, 2459–2472. https://doi.org/10.1007/s40519-022-01385-8
WSSQ - Persian
WSSQ - PersianWSSQ - Turkish
WSSQ - TurkishSevincer, G.M., Kaya, A., Bozkurt, S., Akin, E., & Kose, S. (2017). Reliability, validity, and factorial structure of the Turkish version of the Weight Self-Stigma Questionnaire (Turkish WSSQ). Psychiatry and Clinical Psychopharmacology, 27, 386-392. http://doi.org/10.1080/24750573.2017.1379717
Other Measures
Other Measures CommunityACT ADVISOR Measure
ACT ADVISOR MeasureACT ADVISOR
ACT ADVISOR is a hexaflex-based self-report measure of psychological flexibility, its name being an acronym for the hexaflex processes (Acceptance; Commitment & Taking action; Attention to present; Defusion; Values Identification; Self as Observer; and Resulting psychological flexibility). It may be used both in case formulation and in tracking progress during therapy.
On being presented with this “double hexaflex” diagram, users are asked to choose where they would place themselves on the six different scales representing these core ACT processes, each with “opposite” statements at either end. Scoring is simply a matter of recording the user’s numerical responses and totalling them to give their Resulting psychological flexibility score. If ACT ADVISOR is administered repeatedly, scores can be tracked using the charts provided.
The idea for using the hexaflex as a diagnostic/ case formulation tool was, I believe, originally Kelly Wilson's and his materials (see The Hexaflex Dimensional Approach to Diagnostics) influenced the development of this instrument. Steve Hayes made helpful suggestions about the anchor statements for each process in earlier drafts, and I am also grateful for the ACT listserv community’s interest and input.
ACT ADVISOR statement rating form offers an alternative format. In this version users are asked to rate 12 statements independently of each other and without the possible steer of the double hexaflex diagram. Instructions for scoring this version are provided separately, with the Resulting psychological flexibility score here being converted to a percentage.
ACBS members login their account to see attachments.
Submitted by David Chantry
ACT Advisor - Swedish
ACT Advisor - SwedishACT Advisor Svenska: https://contextualscience.org/files/ACT.Case_.Concepualisation.svens%20ka.Livheim.%C3%B6vers.2016.04.20.pdf
Adult OCD Impact Scale (AOIS)
Adult OCD Impact Scale (AOIS)Wetterneck, C. et al. (2020) Development and validation of the Adult OCD Impact Scale (AOIS): A measure of psychosocial functioning for adults with obsessive-compulsive disorder. Journal of Contextual Behavioral Science, 18, 287-293. https://doi.org/10.1016/j.jcbs.2020.10.005 The AOIS is in the Appendix.
Brief COPE
Brief COPECarver, C.S. (1997) You want to measure coping but your protocol’ too long: Consider the brief cope. Int. J. Behav. Med., 4, 92. https://doi.org/10.1207/s15327558ijbm0401_6
The Brief COPE is available at miami.edu.
Brief COPE - Arabic
Brief COPE - ArabicAlghamdi, M. (2020) Cross-cultural validation and psychometric properties of the Arabic Brief COPE in Saudi population. Medical Journal of Malaysia, 75, 5, 502-509. Full text available on journal website.
Brief COPE - Chinese
Brief COPE - ChineseShao Di, Gao Qingling, Guo Wei (2015). Analysis of reliability and validity of Brief COPE in adolescents experienced explosion events. Journal: Chinese Nursing Research, 34, 4249-4253.
YU Pengpeng, YUAN Lu, WANG Dongfang, Bob Lew, PING Fan, JIA Cunxian (2019) Reliability and validity of Brief COPE Scale in medical college students. Journal of Shandong University(Health Sciences), 2019(01), 101-106
Brief COPE - Dutch
Brief COPE - DutchMarije Dollen, Gert-Jan Pepping, Bob Grove (2015) A comparison of coping-styles of individual and team athletes of Australia and the Netherlands. International Sports Studies.
Brief COPE - French
Brief COPE - FrenchBaumstarck, K., Alessandrini, M., Hamidou, Z. et al. (2017). Assessment of coping: a new french four-factor structure of the brief COPE inventory. Health and Quality of Life Outcomes, 15, 8. https://doi.org/10.1186/s12955-016-0581-9
Muller, L., Spitz, E. (2003). Multidimensional assessment of coping: Validation of the Brief COPE among French population. Encephale, 29(6), 507-518.
Brief COPE - German
Brief COPE - GermanKnoll, N., Rieckmann, N., & Schwarzer, R. (2005). Coping as a mediator between personality and stress outcomes: A longitudinal study with cataract surgery patients. European Journal of Personality, 19, 229-247.
The Brief COPE in German is available on miami.edu
Brief COPE - Greek
Brief COPE - GreekKapsou, M., Panayiotou, G., Kokkinos, C. M., & Demetriou, A. G. (2010). Dimensionality of coping: an empirical contribution to the construct validation of the brief-COPE with a Greek-speaking sample. Journal of health psychology, 15(2), 215–229. https://doi.org/10.1177/1359105309346516
The Brief COPE - Greek is available on miami.edu
Brief COPE - Italian
Brief COPE - ItalianMonzani, D., Steca, P., Greco, A., D'Addario, M., Cappelletti, E., & Pancani, L. (2015). The Situational Version of the Brief COPE: Dimensionality and Relationships With Goal-Related Variables. Europe's journal of psychology, 11(2), 295–310. https://doi.org/10.5964/ejop.v11i2.935
Brief COPE - Japanese
Brief COPE - JapaneseYasumasa Otsuka (2008). 理論的作成方法によるコーピング尺度--COPE [The COPE inventory: a theoretically based coping questionnaire]. Hiroshima psychological research (8), 121-128. http://doi.org/10.15027/26794
Brief COPE - Korean
Brief COPE - KoreanKim, Y., & Seidlitz, L. (2002). Spirituality moderates the effect of stress. Personality and Individual Differences, 32(8), 1377-1390. https://doi.org/10.1016/S0191-8869(01)00128-3
The Brief COPE - Korean is available on miami.edu
Brief COPE - Malay
Brief COPE - MalayYusoff, N., Low, W.Y. & Yip, C.H. (2009) RELIABILITY AND VALIDITY OF THE MALAY VERSION OF BRIEF COPE SCALE: A STUDY ON MALAYSIAN WOMEN TREATED WITH ADJUVANT CHEMOTHERAPY FOR BREAST CANCER. Malaysian Journal of Psychiatry, 18 (1), 1-9.
Muhamad Saiful Bahri Yusoff (2011) The Validity of the Malay Brief COPE in Identifying Coping Strategies among Adolescents in Secondary School. International Medical Journal, 18(1), 29 - 33. The Brief COPE items translation is in Table 1.
Brief COPE - Norwegian
Brief COPE - NorwegianHoel, Geirdal AØ. Belastning, mestring og psykisk helse hos pårørende til mennesker med ruslidelse. Sykepleien Forskning. 2016 http://doi.org/10.4220/Sykepleienf.2016.59839
Kristiansen, E., Roberts, G. C., & Abrahamsen, F. E. (2008). Achievement involvement and stress coping in elite wrestling. Scandinavian journal of medicine & science in sports, 18(4), 526–538. https://doi.org/10.1111/j.1600-0838.2007.00646.x
Brief COPE - Persian
Brief COPE - PersianAshktorab, T., Baghcheghi, N., Seyedfatemi, N., & Baghestani, A. (2017). Psychometric parameters of the Persian version of the BriefCOPE among wives of patients under hemodialysis. Medical journal of the Islamic Republic of Iran, 31, 20. https://doi.org/10.18869/mjiri.31.20
Brief COPE - Portuguese
Brief COPE - PortugueseBrasileiro, S. V., Orsini, M. R., Cavalcante, J. A., Bartholomeu, D., Montiel, J. M., Costa, P. S., & Costa, L. R. (2016). Controversies Regarding the Psychometric Properties of the Brief COPE: The Case of the Brazilian-Portuguese Version "COPE Breve". PloS one, 11(3), e0152233. https://doi.org/10.1371/journal.pone.0152233
Dias, C., Cruz, J. F., & Fonseca, A. M. (2009). Anxiety and coping strategies in sport contexts: a look at the psychometric properties of Portuguese instruments for their assessment. The Spanish journal of psychology, 12(1), 338–348. https://doi.org/10.1017/s1138741600001736
Brief COPE - Sinhala
Brief COPE - SinhalaWeeratunga E, Senadheera C, Hettiarachchi M, Perera B. (2021). Validation of the Sinhalese Version of Brief COPE Scale for patients with cancer in Sri Lanka. BMC Psychology, 10, 157. DOI: 10.1186/s40359-022-00863-z
Brief COPE - Spanish
Brief COPE - SpanishGarcía, F. E., Barraza-Peña, C. G., Wlodarczyk, A., Alvear-Carrasco, M., & Reyes-Reyes, A. (2018). Psychometric properties of the Brief-COPE for the evaluation of coping strategies in the Chilean population. Psicologia, reflexao e critica : revista semestral do Departamento de Psicologia da UFRGS, 31(1), 22. https://doi.org/10.1186/s41155-018-0102-3
Vargas-Manzanares, Sandra Paola; Herrera-Olaya, Gina Paola; Rodríguez-García, Laura; Sepúlveda Carrillo, Gloria Judith (2010) Confiabilidad del cuestionario Brief COPE Inventory en versión en español para evaluar estrategias de afrontamiento en pacientes con cáncer de seno [Reliability of the Questionnaire Brief COPE Inventory in Spanish Version for Assessing Coping Strategies in Patients with Breast Cancer]. Investigación en Enfermería: Imagen y Desarrollo, 12, 1, 7-24. https://www.redalyc.org/pdf/1452/145216903002.pdf
Perczek, R., Carver, C. S., Price, A. A., & Pozo-Kaderman, C. (2000). Coping, mood, and aspects of personality in Spanish translation and evidence of convergence with English versions. Journal of personality assessment, 74(1), 63–87. https://doi.org/10.1207/S15327752JPA740105
The Brief COPE Spanish Translation is available at miami.edu.
Brief COPE - Urdu
Brief COPE - UrduAsma Nisa & Salma Siddiqui (2020) Urdu Translation and Adaptation of Brief COPE Scale. Pakistan Journal of Psychological Research, 35(1), 1-21. https://doi:org/10.33824/PJPR.2020.35.1.1 The Urdu Version of the Brief COPE can be found on psychologyroots.com
Brief COPE - Vietnamese
Brief COPE - VietnameseShoko Matsumoto, et al. (2020). Validation of the Brief Coping Orientation to Problem Experienced (Brief COPE) inventory in people living with HIV/AIDS in Vietnam. Global Health & Medicine, 2(6), 374-383. https://doi.org/10.35772/ghm.2020.01064
COPE
COPEReference: Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology, 56(2), 267-283.
Description from abstract of original paper:
"We developed a multidimensional coping inventory to assess the different ways in which people respond to stress. Five scales (of four items each) measure conceptually distinct aspects of problem-focused coping (active coping, planning, suppression of competing activities, restraint coping, seeking of instrumental social support); five scales measure aspects of what might be viewed as emotion-focused coping (seeking of emotional social support, positive reinterpretation, acceptance, denial, turning to religion); and three scales measure coping responses that arguably are less useful (focus on and venting of emotions, behavioral disengagement, mental disengagement). Study 1 reports the development of scale items. Study 2 reports correlations between the various coping scales and several theoretically relevant personality measures in an effort to provide preliminary information about the inventory's convergent and discriminant validity. Study 3 uses the inventory to assess coping responses among a group of undergraduates who were attempting to cope with a specific stressful episode. This study also allowed an initial examination of associations between dispositional and situational coping tendencies."
COPE - Arabic
COPE - ArabicFahmi H. Fadhel (2015). Psychometric Properties of COPE Inventory in a Yemeni Sample. http://dx.doi.org/10.12785/JEPS/160119
COPE - Chinese
COPE - ChineseZhang Weidong. (2001). STUDY ON THE DIMENSIONALITY OF THE COPING INVENTORY(COPE). Acta Psychologica Sinica, 33(01), 55-62. http://journal.psych.ac.cn/acps/EN/Y2001/V33/I01/55
COPE - Croatian
COPE - CroatianHudek-Knežević, J., Kardum, I. and Vukmirović, Ž. (1999). The structure of coping styles: a comparative study of croatian sample. Eur. J. Pers., 13, 149-161. https://doi.org/10.1002/(SICI)1099-0984(199903/04)13:2<149::AID-PER326>3.0.CO;2-Z
COPE - Dutch
COPE - DutchKleijn, W. C., van Heck, G. L., & van Waning, A. (2000). Ervaringen met een Nederlandse bewerking van de COPE copingvragenlijst. De COPE-Easy [Experiences with a Dutch adaptation of the COPE coping questionnaire: The COPE-Easy]. Gedrag & Gezondheid: Tijdschrift voor Psychologie en Gezondheid, 28(4), 213–226.
COPE - Estonian
COPE - EstonianKallasmaa, T. & Pulver, A. (2000) The structure and properties of the Estonian COPE inventory. Personality and Individual Differences, 29(5), 881-894. https://doi.org/10.1016/S0191-8869(99)00240-8
COPE - Greek
COPE - GreekMagda Dinou, Despina Moraitou, Georgia Papantoniou, Anastasia Kalogiannidou, Aphrodite Papantoniou (2013) Ψυχομετρικές ιδιότητες της ελληνικής εκδοχής του Ερωτηματολογίου Προσανατολισμών στην Αντιμετώπιση Προβλημάτων [Psychometric properties of the Greek version of the Coping Orientations to Problems Experienced - COPE Inventory]. Scientific Annals - School of Psychology AUTh, 10, 163-192. http://ejournals.lib.auth.gr/psyannals/article/view/4270
COPE - Italian
COPE - ItalianClaudio Sica, Caterina Novara, Stella Dorz, & Ezio Sanavio (1997) Coping strategies: Evidence for cross-cultural differences? A preliminary study with the Italian version of coping orientations to problems experienced (COPE). Personality and Individual Differences, 23(6), 1025-1029. https://doi.org/10.1016/S0191-8869(97)00112-8
COPE - Japanese
COPE - JapaneseYasumasa Otsuka (2008). 理論的作成方法によるコーピング尺度--COPE [The COPE inventory: a theoretically based coping questionnaire]. Hiroshima psychological research (8), 121-128. http://doi.org/10.15027/26794 The Japanese COPE items are in table 2.
COPE - Latvian
COPE - LatvianPetrova, I. (2009) Paškategorizācijas, uztvertā stresa un stresa pārvarēšanas stratēģiju saistība ar bezdarbnieku priekšstatiem par izredzēm atgriezties darba tirgū. Thesis. http://dspace.lu.lv/dspace/handle/7/9975
COPE - Portuguese
COPE - PortugueseCabral, J., & Mena Matos, P. (2010). Cope-inventory: Teste da estrutura factorial com uma amostra de jovens adultos universitários. PSICOLOGIA, 24(1), 49–71. https://doi.org/10.17575/rpsicol.v24i1.296
COPE - Romanian
COPE - RomanianCraovan, D.I. & Sava, Florin. (2013). Translation, adaptation, and validation on romanian population of cope questionnaire for coping mechanisms analysis. Cognition, Brain, Behavior, 17, 61-76. The Romanian version of the COPE is in the appendix.
COPE - Russian
COPE - RussianRasskazova, E. I., Gordeeva, T. O., & Osin, E. N. (2013). Koping-strategii v strukture deyatel'nosti i samoregulyatsii: psikhometricheskie kharakteristiki i vozmozhnosti primeneniya metodiki COPE [Coping Strategies in the Structure of Activity and Self-Regulation: Psychometric Properties and Applications of the COPE Inventory]. Psychology. Journal of Higher School of Economics, 10(1), 82-118. (in Russian) https://psy-journal.hse.ru/ru/2013-10-1/78932127.html
COPE - Serbian
COPE - SerbianThe COPE Serbian Transation and the Brief COPE Serbian Translation can be found on the Repository of psychological instruments in Serbian [Repozitorijum psiholoških instrumenata na srpskom jeziku] (REPOPSI). https://doi.org/10.17605/OSF.IO/5ZB8P
COPE - Slovak
COPE - SlovakHalamová, J., Kanovský, M., Krizova, K., et al. (2021). The Factor Structure and External Validity of the COPE 60 Inventory in Slovak Translation. Frontiers in Psychology, 12, 800166. DOI: 10.3389/fpsyg.2021.800166
COPE - Spanish
COPE - SpanishThe COPE in Spanish is available at https://local.psy.miami.edu/people/faculty/ccarver/availbale-self-report-instruments/cope/cope-in-spanish/
COPE - Turkish
COPE - TurkishMehmet Yücel AĞARGÜN, Lütfullah BEŞİROĞLU, Ümit Kemal KIRAN, Ömer Akil ÖZER, Hayrettin KARA (2005) COPE (Başa Çıkma Tutumlarını Değerlendirme Ölçeği): Psikometrik özelliklere ilişkin bir ön çalışma [The psychometric properties of the COPE inventory in Turkish
sample: a preliminary research]. Anatolian Journal of Psychiatry, 6, 221-226. Full text of the article is on www.researchgate.net
COPE - Ukrainian
COPE - UkrainianKovalenko, Y.V. (2019). Adaptation and validation of the Ukrainian dispositional ‘cope’ questionnaire. Університет імені Альфреда Нобеля (Alfred Nobel University), Серія «Педагогіка і психологія». Педагогічні науки, 2 (18). http://doi.org/10.32342/2522-4115-2019-2-18-9
Emotion Efficacy Scale (EES2) - Revised
Emotion Efficacy Scale (EES2) - RevisedOverview
The Emotion Efficacy Scale (EES2) assesses the degree to which people can respond to a full range of emotions in a contextually-sensitive, values-consistent manner. The original version of the scale was first published in Emotion Efficacy Therapy (McKay & West, 2016). It has since been revised and validated in English, Farsi and Turkish. (See references below).
Professionals can use the scale in conjunction with administering the Emotion Efficacy Therapy protocol in a group or individual format, or as an adjunct to increasing emotional intelligence, psychological flexibility, and resilience in clinical or coaching work.
This scale has been validated for adults ages 18 and older.
Developer
Aprilia West, PsyD, MT, PCC
Scoring/ Interpretation
10 items total
Items 3-8 are reverse scored
Score can range from 10-50
Items are summed; a higher score indicates higher emotion efficacy
Percentile Rankings
Based on a validation study (n=24) with a clinical population:
Total score >19: 25th percentile
Total score >25: 50th percentile
Total score >31: 75th percentile
Total score >37: 90th percentile
Use of this scale
No permission is needed to use this scale for clinical purposes. If you are using this scale in conjunction with research, please notify aprilia@drapriliawest.com.
Download the EES2 below for the most recent version of the scale and for scoring instructions.
Learn More:
Bozkurt, F., Uzun, R. B., & West, A. (2024). Psychometric Properties of the Turkish Version of the Emotion Efficacy Scale– 2 in a Sample of Turkish Emerging Adults. Emerging Adulthood, 0(0). https://doi.org/10.1177/21676968241247878.
Foroughi, A. A., Parvizifard, A., Sadeghi, K., & Moghadam, A. P. (2021). Psychometric properties of the Persian version of the Emotion Regulation Questionnaire. Trends in psychiatry and psychotherapy, 43(2), 101–107. https://doi.org/10.47626/2237-6089-2018-0106.
Shannon, M. (2018). Measuring Emotion Regulation, Psychological Flexibility and Valued Living through the Emotion Efficacy Scale: A Validation Study. The Wright Institute, Berkeley California.
www.emotionefficacytherapy.com
Forms of Responding to Self-Critical Thoughts Scale’ (FoReST)
Forms of Responding to Self-Critical Thoughts Scale’ (FoReST)White, R.G., Larkin, P., McCluskey, J., Lloyd, J., & McLeodd, H.J. (2020). The development of the ‘Forms of Responding to Self-Critical Thoughts Scale’ (FoReST). Journal of Contextual Behavioral Science, 15, 20-29. https://doi.org/10.1016/j.jcbs.2019.11.003
FoReST - Turkish
FoReST - TurkishMehmet Emrah Karadere & Huseyin Sehid Burhan (2021) Turkish Version of the Forms of Responding to Self-Critical Thoughts Scale (FoReST): A Reliability and Validity Analysis over Non-Clinical Samples. Psychiatry and Behavioral Sciences, 11(1):57-62. http://doi.org/10.5455/PBS.20210315025754
The Türkish version of the FoReST is on the ACBS Türkiye Chapter website
Generalized Pliance Questionnaire (GPQ)
Generalized Pliance Questionnaire (GPQ)Ruiz, F.J. et al (2019) Development and initial validation of the Generalized Pliance Questionnaire. Journal of Contextual Behavioral Science, 12, 189-198. https://doi.org/10.1016/j.jcbs.2018.03.003 English and Spanish translations of the GPQ are in the Supplementary material Appendix.
GPQ - Polish
GPQ - PolishDudek, J., Cyniak-Cieciura, M. & Ostaszewski, P. (2023). The Polish adaptation of the measurements of rule-governed behaviors: Generalized Pliance Questionnaire, Generalized Tracking Questionnaire and Generalized Self-Pliance Questionnaire. PLOS ONE, 18(4), e0283795. https://doi.org/10.1371/journal.pone.0283795 The Polish versions of the GPQ, GTQ, and GSPQ are in Table 1.
GPQ - Spanish
GPQ - SpanishRuiz, F. J., Odriozola-González, P., & Suárez-Falcón, J. C. (2020 in press). Psychometric properties of the Generalized Pliance Questionnaire in Spain. European Journal of Psychological Assessment. https://doi.org/10.1027/1015-5759/a000614
Ruiz, F.J. et al (2019) Development and initial validation of the Generalized Pliance Questionnaire. Journal of Contextual Behavioral Science, 12, 189-198. https://doi.org/10.1016/j.jcbs.2018.03.003 The Spanish translation of the GPQ is in the Supplementary material Appendix.
MindFlex Assessment System
MindFlex Assessment System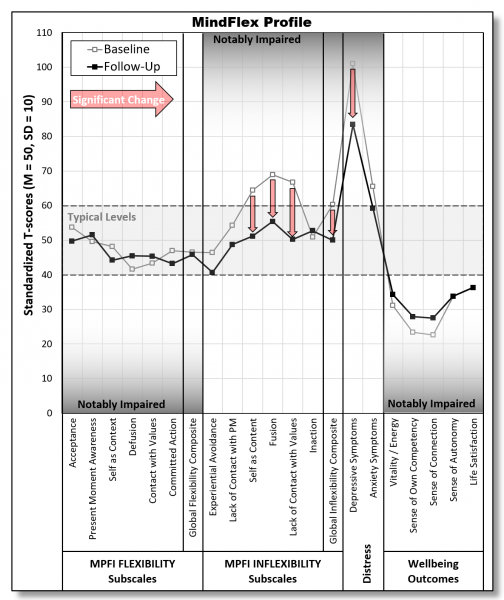
THE SERVICE
The MindFlex Assessment System is an online service designed for therapists using ACT [or Mindfulness-based] interventions. The MindFlex system:
- provides standardized profiles showing how individual clients are functioning across 21 well-validated indices
- provides a straightforward and easy method for therapists to track the process of change in therapy.
The MINDFLEX SYSTEM assesses:
- 7 dimensions of flexibility
- 7 additional dimensions of inflexibility
- 2 main dimensions of psychological distress (depressive & anxiety symptoms)
- 5 dimensions of well-being
HOW TO GET STARTED:
By enrolling yourself as a clinician in the project (2-5min survey) and then enrolling individual clients (3-5min survey), you can have clients complete a 15-20min survey assessing all of these scales.
WEBSITE DETAILING THE SERVICE
Each time a client completes a MindFlex assessment, we will then score the responses, and integrate that information into a standardized profile to show you how that client is doing compared to thousands of others. If that client has completed a previous MindFlex assessment, then the profile generated will help you track statistically significant change.
COST FOR THE SERVICE:
The MindFlex service is entirely free of charge. In fact, roughly the first 100 therapists to help us pilot this service can receive up to $100 in compensation and their clients can receive up to $80 for participating in the MindFlex Assessment Project, conducted by Dr. Ron Rogge.
Mindful Eating Questionnaire (MEQ)
Mindful Eating Questionnaire (MEQ)Framson, C., Kristal, A. R., Schenk, J. M., Littman, A. J., Zeliadt, S., & Benitez, D. (2009). Development and validation of the mindful eating questionnaire. Journal of the American Dietetic Association, 109(8), 1439–1444. https://doi.org/10.1016/j.jada.2009.05.006
MEQ - Brazilian Portuguese
MEQ - Brazilian PortugueseMindful Eating Questionnaire (MEQ) Brazilian Portuguese version
Corresponding author: Paola Lucena-Santos, Ph.D. in Clinical Psychology.
E-mail: paolabc2.lucena@gmail.com
WhatsApp: +55 (51) 998055874
Affiliation: CINEICC - Cognitive Behavioral Research Center (Faculty of Psychology and Education Sciences, University of Coimbra)
MEQ - Chinese
MEQ - ChineseZhang, Q., Hugh-Jones, S. & O'Connor,D.B. (2022). Investigation of psychometric properties of the Mindful Eating Questionnaire in Chinese adolescents and young adults using mixed methods. Appetite, 176, 106097. https://doi.org/10.1016/j.appet.2022.106097
MEQ - Greek
MEQ - GreekKoptsi, I., Tsapekos, D. & Goulis, D. (2022). ADAPTATION OF THE MINDFUL EATING QUESTIONNAIRE IN GREEK. Hellenic Journal of Psychology, 19(1), 1-20. https://doi.org/10.26262/hjp.v19i1.7884
MEQ - Italian
MEQ - ItalianClementi, C., Casu, G., & Gremigni, P. (2017). An Abbreviated Version of the Mindful Eating Questionnaire. Journal of Nutrition Education and Behavior, 49(4), 352–356.e1. https://doi.org/10.1016/j.jneb.2017.01.016
MEQ - Korean
MEQ - KoreanSeung-Hye Choi, Eun-Mi Lee, Hae-Young Lee. (2018). Psychometric Evaluation of Korean Version of Mindful Eating Questionnaire. Journal of the Korean Wellness Society, 13.1, 63-72.
MEQ - Malay
MEQ - MalayAbdul Basir, S.M., Abdul Manaf, Z., Ahmad, M., Abdul Kadir, N.B., Ismail, W.N.K., Mat Ludin, A.F., & Shahar, S. (2021) Reliability and Validity of the Malay Mindful Eating Questionnaire (MEQ-M) among Overweight and Obese Adults. Int. J. Environ. Res. Public Health, 18, 1021. https://doi.org/10.3390/ijerph18031021 Translation is in Appendix A.
MEQ - Persian
MEQ - PersianReferences:
Abbaspoor, Z., Javadifar, N., Miryan, M. et al. (2018) Psychometric properties of the Iranian version of mindful eating questionnaire in women who seeking weight reduction. J Eat Disord 6, 33. https://doi.org/10.1186/s40337-018-0220-4
Rezaei, S. & Jahanbin, E. (2022). Translation and Validation of the Persian Version of Mindful Eating Questionnaire. Caspian Journal of Neurological Sciences, 8(2), 76-89. http://dx.doi.org/10.32598/CJNS.8.29.2
MEQ - Romanian
MEQ - RomanianSerban, D. M., Serban, C. L., Ursoniu, S., Putnoky, S., Moleriu, R. D., & Putnoky, S. (2022). Mindful Eating Questionnaire: Validation and Reliability in Romanian Adults. International Journal of Environmental Research and Public Health, 19(17), 10517. https://doi.org/10.3390/ijerph191710517
MEQ - Turkish
MEQ - TurkishReferences:
Gizem KÖSE, Muhittin TAYFUR, İnci BİRİNCİOĞLU, Aslıhan DÖNMEZ (2016) Yeme Farkındalığı Ölçeği’ni Türkçeye Uyarlama Çalışması [Adaptation Study of the Mindful Eating Questiıonnare (MEQ) into Turkish.] Journal of Cognitive-Behavioral Psychotherapy and Research, 5(3), 125-134. DOI: 10.5455/JCBPR.250644
Kömürcü Akik, B., & Yiğit, İ. (2023). Evaluating the psychometric properties of the mindful eating questionnaire: Turkish validity and reliability study. Curr Psychol, 42, 12661–12670. https://doi.org/10.1007/s12144-021-02502-z
Mindful Eating Questionnaire for Children (MEQ-C)
Mindful Eating Questionnaire for Children (MEQ-C)Kocaadam-Bozkurt, B., Köksal, E. & Özalp Ateş, F.S. (2022). Mindful Eating Questionnaire for Children: Validation and Reliability in Turkish Children. Mindfulness, 13, 1469–1478. https://doi.org/10.1007/s12671-022-01889-5
MEQ-C (Chinese)
MEQ-C (Chinese)Wang, D., Hu, Y., Zhou, H., Ye, Z., & Fu, J. (2022). Translation and Modification of a Mindful Eating Questionnaire for Children Assisted by Item Response Theory in Chinese Children and Adolescents. Nutrients, 14(14), 2854. https://doi.org/10.3390/nu14142854
MEQ-C (Turkish)
MEQ-C (Turkish)Kocaadam-Bozkurt, B., Köksal, E. & Özalp Ateş, F.S. (2022). Mindful Eating Questionnaire for Children: Validation and Reliability in Turkish Children. Mindfulness, 13, 1469–1478. https://doi.org/10.1007/s12671-022-01889-5
New SVS version
New SVS versionWe've also similarly updated the SVS. Please use this version rather than the previously posted one.
Parental Psychological Flexibility Questionnaire (PPF)
Parental Psychological Flexibility Questionnaire (PPF)Burke, K., Moore, S. (2015). Development of the Parental Psychological Flexibility Questionnaire. Child Psychiatry & Human Development, 46, 548–557. https://doi.org/10.1007/s10578-014-0495-x
Personal Values Questionnaire II (PVQII)
Personal Values Questionnaire II (PVQII)We were a bit reluctant to do this as it basically invalidates what little prior data there is for the Personal Values Questionnaire, but it made sense to us under the circumstances.
We’ve gone through two sets of reformatting and rewording the instrument. The first ‘re-draft’ was spurred by Ann Bailey, who rightfully noted that the wording of some of the Likert items was a bit complicated for those with a sub-college writing level and that the ordering of the Likert questions did not flow very well. This re-draft has been up on the ACBS site for a couple of years now.
The most recent changes occurred late last year. In the process of translating the instrument into German, Andrew Gloster and two of his doctoral students at Dresden Technical University noted that the prompts provided for the domain-specific values narratives differed across domains.
I had initially done this to provide a variety of ways of talking about values in the hope that subjects who had not been through ACT therapy might still ‘get’ what a value is. Andrew, I think rightfully, questioned this strategy as the different prompts might differentially cue different qualities of responses across domains, resulting in narratives (and subsequently, Likert ratings on those narratives) that might be functionally different.
So, in advance of that translation, we decided on a uniform values narrative prompt to be used across all domains. That served as the basis for the German translation, which I’ve also attached. I’m posting both of these on the ACBS site, but wanted to send them here as well as I know some others have used or plan to use the PVQ for research, etc (Martin Cernval from Uppsala University will be beginning a Swedish translation soon, for example).
I thought about further modifying the instrument (e.g., I really like Kelly Wilson’s addition of Parenting and Aesthetics values domains to the VLQ), but the instrument is beastly enough already. Functionally, it’s still the same instrument—except, hopefully, the aspects of the original instrument that functioned to confuse some subjects and potentially yield differentially ‘ACT-consistent’ (for lack of a better phrase) across domains have been eliminated!
PVQ II - German
PVQ II - German CommunityPVQ II - Japanese
PVQ II - JapanesePersonal Values Questionnaire II (PVQ II) is a scale that measures the value of "value", which is the core process of ACT, and the behavior along with the value in each area of life. PVQⅡ has an 8-item 3-factor structure.
Rimi Doi, Kengo Yokomitsu, Yuji Sakano (2014). Verification of the internal consistency and validity of Personal Values Questionnaire II. Behavior Therapy Research, 40 (1), 45-55.
The PVQ II Japanese version is on the ACBS Japan Chapter website.
PVQ-II - Spanish
PVQ-II - SpanishEn adjunto está la traducción y adaptación al español del PVQ-II (que está en esta página). La traducción fue realizada por Solange Estévez y Dalila Acuña, del equipo de diseminación de Grupo ACT Argentina (https://grupoact.com.ar/el-cuestionario-de-valores-personales-ii/)
Tiene algunas adaptaciones menores de formato respecto al original en inglés (como separar las puntuaciones de las descripciones en las escalas Likert), y está en castellano neutro.
Personal Values Questionnaire (PVQ)
Personal Values Questionnaire (PVQ)This is a new approach developed by J. T. Blacklege and Joe Ciarocchi at the University of Wollongong.
In an August 2005 email J. T. said this:
Joseph Ciarrochi & I (with invaluable suggestions from Steve) have just finished designing two new ACT values questionnaires that borrow elements from Sheldon's Personal Striving assessment form (Joseph discovered Kennon Sheldon's work a while back and it pointed us in a direction we felt might enhance ACT values assessment). One is a full-length form called the Personal Values Questionnaire (which measures all 9 ACT values domains); the second is called the Social Values Survey (which measures only social, family, and couples relationships) that we tailored for a brief intervention with young adolescents.
There is currently no psychometric data for either (they are changed enough that Sheldon's Personal Striving data is largely irrelevant), though we will be validating the SVS on a sample of 8th graders in a few weeks, and validating the PVQ on a university student sample early next year. Please feel more than free to validate these questionnaires on any samply you see fit (just let us know--we'd love to see the data). The format of the questionnaire is close enough to Sheldon's for us to expect the measures to have similarly reasonable psychometric properties, but, of course, who knows until we see data.
We had two primary purposes in mind while we were designing these instruments. First, we wanted to describe each values domain in a way likely to influence subjects to write relatively ACT-consistent values--even if these subjects had not been exposed to ACT therapy. As we all know, ACT talks about values in a different way than the term is usually used--and it's thus hard to expect someone not familiar with ACT to state a value in an ACT-consistent way without interacting with a therapist. We wanted to make it clear to subjects that by value, we are referring to unilateral actions that are likely to lead to increased vitality, meaning, purpose--not static end states that appear implicitly out of one's control. In other words, to avoid getting responses like "I value close friendships", we included prompts like, "What kinds of friendships would you most like to build? If you were able to be the best friend possible, how would you behave toward your friends? For example, you might value building friendships that are supportive, considerate, caring, accepting, loyal, or honest—but choose for yourself which qualities you would most like to bring to your friendships.
Some subtle changes from wording used on previous versions of values questionnaires, but we felt the 'build' theme, along with examples, seemed to provide the kind of prompts that might be more helpful. Second, we wanted to include Likert-scale questions that assessed things like how much each stated value might be a function of things like pliance or experiential avoidance. Steve oriented us back toward RFT/rule governed behaviour terms that capture what we were trying to assess: as it stands now, question one under each values domain on the SVS and PVQ assesses pliance, question 2 assesses avoidant tracking, and questions 3 & 4 assess augmentals. There are also items that get at importance of each value, effectiveness in moving toward it, etc. As it stands (using Sheldon's scoring algorithms and common sense), subtracting the sum of items 1 & 2 from the sum of items 3 & 4 would yield a sort of 'value purity' score that tells us to what degree a subject/client values the stated value for the reasons we'd hope for from an ACT perspective (higher positive score = greater 'purity' of the value; negative score means the 'value' is actually a function of pliance and/or avoidance).
Psychological Flexibility Questionnaire
Psychological Flexibility QuestionnaireBen-Itzhak, S., Bluvstein, I., & Maor, M. (2014). The Psychological Flexibility Questionnaire (PFQ): Development, Reliability and Validity. WebmedCentral PSYCHOLOGY, 5(4), WMC004606. DOI: 10.9754/journal.wmc.2014.004606
Questionnaire on Self-Transcendence
Questionnaire on Self-TranscendenceThis scale, informed by ACT and other contextual cognitive behavioral therapies, measures three related factors:
1. Distancing from content of mental experience (informed by cognitive defusion)
2. Observing self - capacity to "notice the noticer" of experiences (informed by self-as-context)
3. Inter-transcendence - capacity to recognize transcendent connection between self and other beings (informed by aspects of self-as-context and RFT)
The scale is available for public use.
Please cite the scale as follows:
Fishbein, J. N., Baer, R. A., Correll, J., & Arch, J. J. (2020). The Questionnaire on Self-Transcendence (QUEST): A measure of trait self-transcendence informed by contextual cognitive behavioral therapies. Assessment, In press. https://doi.org/10.1177/1073191120980061
Scale for Personality Rigidity
Scale for Personality RigidityScale for personality rigidity.
Reference: Rehfisch, J.M. (1958). A scale for personality rigidity. Journal of Consulting Psychology, 22, 11-15.
This scale has been found to relate to rule governed behavior in laboratory studies.
Wulfert, E., Greenway, D. E., Farkas, P., Hayes, S. C., & Dougher, M. J. (1994). Correlation between a personality test for rigidity and rule-governed insensitivity to operant contingencies. Journal of Applied Behavior Analysis, 27, 659-671.
From abstract:
"Adults were selected on the basis of their scores on the Scale for Personality Rigidity (Rehfisch, 1958). Their scores served as a measure of hypothesized rule governance in the natural environment. Experiment 1 studied the effects of accurate versus minimal instructions and high versus low rigitidy on performance on a multiple differential-reinforcement-of-low-rate (DRL) 4-s fixed-ratio (FR) 18 schedule. When the schedule was switched to extinction, accurate instructions and high rigidity were associated with greater perseveration in the response pattern subjects developed during the reinforcement phase. In Experiment 2, the effects of rigidity and of accurate versus inaccurate instructions were studied. Initially, all subjects received accurate instructions about an FR schedule. The schedule was then switched to DRL, but only half of the subjects received instructions about the DRL contingency, and the other half received FR instructions as before. Accurate instructions minimized individual differences because both high and low scorers on the rigidity scale earned points in DRL. However, when inaccurate instructions were provided, all high-rigidity subjects follow them although they did not earn points on the schedule, whereas most low-rigidity subjects abandoned them and responded appropriately to DRL. The experiments demonstrate a correlation between performances observed in the human operant laboratory and a paper-and-pencil test of rigidity that purportedly reflects important response styles that differentiate individuals in the natural environment. Implications for applied research and intervention are discussed."
Tacting of Function Scale (TOF)
Tacting of Function Scale (TOF)Pierce, B.G. & Levin, M.E. (2019). Preliminary validation and reliability assessment of a 10-item Tacting of Function Scale. Journal of Contextual Behavioral Science, 12, 322-328. https://doi.org/10.1016/j.jcbs.2019.01.002 The Tacting of Function Scale can be downloaded from the Utah State University ACT Research Group.
Teacher Psychological Flexibilty Scale (TPFS)
Teacher Psychological Flexibilty Scale (TPFS)Teacher Psychological Flexibilty Scale was developed in Turkish.
Çelik Aslan, H. & Tuzgöl Dost, M. (2023). ÖĞRETMEN PSİKOLOJİK ESNEKLİK ÖLÇEĞİ’ NİN GELİŞTİRİLMESİ [DEVELOPMENT OF THE TEACHER PSYCHOLOGICAL FLEXIBILITY SCALE]. Elektronik Sosyal Bilimler Dergisi, 22(85), 86-102. DOI: 10.17755/esosder.1197849
Thought Control Questionnaire
Thought Control QuestionnaireThe Thought Control Questionnaire assesses different methods used to control unwanted/aversive thoughts. The measure can be downloaded here.
Reference: Wells, A., & Davies, M. I. (1994). The thought control questionnaire: A measure of individual differences in the control of unwanted thoughts. Behaviour Research and Therapy, 32, 871–878.
Toronto Alexithymia Scale (TAS-20)
Toronto Alexithymia Scale (TAS-20)Authors: R. Michael Bagby, James D. A. Parker and Graeme J. Taylor
The TAS is a 20-item instrument that is one of the most commonly used measures of alexithymia. Alexithymia refers to people who have trouble identifying and describing emotions and who tend to minimise emotional experience and focus attention externally.
The TAS-20 has 3 subscales:
• Difficulty Describing Feelings subscale is used to measure difficulty describing emotions. 5 items – 2, 4, 11, 12, 17.
• Difficulty Identifying Feeling subscale is used to measure difficulty identifying emotions. 7 items – 1, 3, 6, 7, 9, 13, 14.
• Externally-Oriented Thinking subscale is used to measure the tendency of individuals to focus their attention externally. 8 items – 5, 8, 10, 15, 16, 18, 19, 20.
Scoring: The TAS-20 is a self-report scale that is comprised of 20 items. Items are rated using a 5-point Likert scale whereby 1 = strongly disagree and 5 = strongly agree. There are 5 items that are negatively keyed (items 4, 5, 10, 18 and 19). The total alexithymia score is the sum of responses to all 20 items, while the score for each subscale factor is the sum of the responses to that subscale. The TAS-20 uses cutoff scoring: equal to or less than 51 = non-alexithymia, equal to or greater than 61 = alexithymia. Scores of 52 to 60 = possible alexithymia.
Reliability: Demonstrates good internal consistency (Cronbach’s alpha = .81) and test-retest reliability (.77, p<.01). Validity: Research using the TAS-20 demonstrates adequate levels of convergent and concurrent validity. The 3 factor structure was found to be theoretically congruent with the alexithymia construct. In addition, it has been found to be stable and replicable across clinical and nonclinical populations.
Reference: Bagby, R. M., Parker, J. D. A. & Taylor, G. J. (1994). The twenty-item Toronto Alexithymia Scale-I. Item selection and cross-validation of the factor structure. Journal of Psychosomatic Research, 38, 23-32." Information quoted from Ciarrochi, J. & Bilich, L. (2006). Process measures of potential relevance to ACT. Unpublished manuscript, University of Wollongong, Australia.
Please see http://www.gtaylorpsychiatry.org/tas.htm for additional details.
TAS-20 - Albanian
TAS-20 - AlbanianArenliu, A., Krasniqi, B., Kelmendi, K., & Statovci, S. (2021). Exploring Factor Validity of 20-Item Toronto Alexithymia Scale (TAS-20) in Albanian Clinical and Nonclinical Samples. SAGE Open. https://doi.org/10.1177/2158244020988726
TAS-20 - Arabic
TAS-20 - ArabicEl Abiddine, F. Z., Dave, H., Aldhafri, S., El-Astal, S., Hemaid, F., & Parker, J. D. A. (2017). Cross-validation of the 20-item Toronto Alexithymia Scale: Results from an Arabic multicenter study. Personality and Individual Differences, 113, 219–222. https://doi.org/10.1016/j.paid.2017.03.017
TAS-20 - Bulgarian
TAS-20 - BulgarianPopov, V., Psederska, E., Peneva, E., Bozgunov, K., Vasilev, G., Nedelchev, D., & Vassileva, J. (2016). Psychometric Characteristics of the Bulgarian Version of the Toronto Alexithymia Scale (TAS-20). Psychological Research, 19(2), 25-42. The Bulgarian translation of the TAS-20 items is in table 1. The full text of the article can be found at venpopov.com
TAS-20 - Chinese
TAS-20 - ChineseYUAN Yonggui, SHEN Zuohua, ZHANG Xiangrong, WU Aiqin, SUN Houchun, ZHANG Ning, ZHANG Xinbao, LI Hailin (2003) The reliability and validity of Toronto alexithymia scale (TAS - 20). SICHUAN MENTAL HEALTH, Year: 2003 Issue: 1, 25-27.
Xiongzhao Zhu, Jinyao Yi, Shuqiao Yao, Andrew G. Ryder, Graeme J. Taylor, & R. Michael Bagby (2007) Cross-cultural validation of a Chinese translation of the 20-item Toronto Alexithymia Scale. Comprehensive Psychiatry, 48(5), 489-496. https://doi.org/10.1016/j.comppsych.2007.04.007
Ling, Y., Zeng, Y., Yuan, H., & Zhong, M. (2016). Cross-cultural validation of the 20-item Toronto Alexithymia Scale in Chinese adolescents. Journal of psychiatric and mental health nursing, 23(3-4), 179–187. https://doi.org/10.1111/jpm.12298
TAS-20 - Croatian
TAS-20 - CroatianKusevic, Z., Civljak, M., Rukavina, T. V., Babic, G., Loncar, M., Cusa, B. V., & Gregurek, R. (2013). The Connection between Alexithymia and Somatic Morbidity in a Population of Combat Veterans with Chronic PTSD. Acta informatica medica: AIM: journal of the Society for Medical Informatics of Bosnia & Herzegovina, 21(1), 7–11. https://doi.org/10.5455/AIM.2013.21.7-11
TAS-20 - Czech
TAS-20 - CzechAnna Faltýnková (2018) Souvislost alexithymie a závislosti na online hraní. Thesis. The Czech version of the TAS-20 is in the Appendix.
TAS-20 - Dutch
TAS-20 - DutchKooiman, C. G., Spinhoven, P., & Trijsburg, R. W. (2002). The assessment of alexithymia. A critical review of the literature and a psychometric study of the Toronto Alexithymia Scale-20. Journal of Psychosomatic Research, 53, 1083-1090. http://doi.org/10.1016/S0022-3999(02)00348-3
Meganck, R., Vanheule, S., & Desmet, M. (2008). Does the TAS-20 measure alexithymia? A study of natural language use. 28th European Conference on Psychosomatic Research, Abstracts. Presented at the 28th European Conference on Psychosomatic Research (ECPR - 2012).
Inslegers, R., Meganck, R., Ooms, E., Vanheule, S., Bagby, M., Taylor, G., De Fruyt, F., et al. (2013). The Dutch language version of the Toronto structured interview for Alexithymia: reliability, concurrent validity, and factor structure. PSYCHOLOGICA BELGICA, 53(1), 93–116.
TAS-20 - Finnish
TAS-20 - FinnishMatti Joukamaa, Jouko Miettunen, Pirkko Kokkonen, Minna Koskinen, Juhani Julkunen, Jussi Kauhanen, Jari Jokelainen, Juha Veijola, Kristian Läksy, Marjo-Riitta Järvelin (2001). Psychometric properties of the Finnish 20-item Toronto Alexithymia Scale. Nordic Journal of Psychiatry, 55(2), 123-127. http://doi.org/10.1080/08039480116694
Säkkinen, P. et al. (2007) Psychometric Properties of the 20-Item Toronto Alexithymia Scale and Prevalence of Alexithymia in a Finnish Adolescent Population. Psychosomatics, 48 (2), 154-161. https://doi.org/10.1176/appi.psy.48.2.154
TAS-20 - French
TAS-20 - FrenchWatters, C.A., Taylor, G.J., Ayearst, L., Bagby, R.M. (2019) Measurement invariance of English and French language versions of the 20-item Toronto Alexithymia Scale. European Journal of Psychological Assessment, 35, 29-36.
Loas, G., Fremaux, D., & Marchand, M. P. (1995). Etude de la structure factorielle et de la cohérence interne de la version française de l'échelle d'alexithymie de Toronto à 20 items (TAS-20) chez un groupe de 183 sujets sains [Factorial structure and internal consistency of the French version of the twenty-item Toronto Alexithymia Scale in a group of 183 healthy probands]. L'Encephale, 21(2), 117–122.
Loas G., Otmani O., Verrier A., Fremaux D. & Marchand M.P. (1995) Factor Analysis of the French Version of the 20-ltem Toronto Alexithymia Scale (TAS-20). Psychopathology, 29, 139–144. https://doi.org/10.1159/000284983
TAS-20 - German
TAS-20 - GermanGrabe, H.J., Löbel, S, Dittrich, D., Bagby, R.M., Taylor, G.J., Quilty, L.C., Spitzer, C., Barnow, S., Mathier, F., Jenewein, J., Freyberger, H.J., Ruffer, M. (2009). The German Version of the Toronto Structured Interview for Alexithymia: Factor Structure, Reliability, and Concurrent Validity in a Psychiatric Patient Sample. Comprehensive Psychiatry, 50, 424-430.
Bach, M., Bach, D., de Zwaan, M., & Serim, M. (1996). Validierung der deutschen Version der 20-Item Toronto-Alexithymie-Skala bei Normalpersonen und psychiatrischen Patienten [Validation of the German version of the 20-item Toronto Alexithymia Scale in normal adults and psychiatric inpatients]. PPmP: Psychotherapie Psychosomatik Medizinische Psychologie, 46(1), 23–28.
TAS-20 - Greek
TAS-20 - GreekIoannis Tsaousis, Graeme Taylor, Lena Quilty, Stelios Georgiades, Marios Stavrogiannopoulos, R. Michael Bagby (2010) Validation of a Greek adaptation of the 20-item Toronto Alexithymia Scale. Comprehensive Psychiatry, 51(4), 443-448. https://doi.org/10.1016/j.comppsych.2009.09.005 Full text of the article is on psychology.soc.uoc.gr
TAS-20 - Hindi
TAS-20 - HindiPandey, R., Mandal, M.K., Taylor, G.J. & Parker, J.D.A. (1996). Cross-cultural alexithymia: Development and validation of a Hindi translation of the 20-item Toronto alexithymia scale. Journal of Clinical Psychology, 52, 173-176. https://doi.org/10.1002/(SICI)1097-4679(199603)52:2<173::AID-JCLP8>3.0.CO;2-V
TAS-20 - Hungarian
TAS-20 - HungarianCserjesi Renata , Luminet Olivier , Lenard Laszlo (2007) RELIABILITY AND FACTOR VALIDITY OF THE HUNGARIAN TRANSLATION OF THE TORONTO ALEXITHYMIA SCALE IN UNDERGRADUATE STUDENT SAMPLES. Magyar Pszichologiai Szemle (Hungarian Psychological Review), 62,3, 355-368.
Cserjesi, Renata & Luminet, Olivier & Lénárd, László. (2007). A Torontói Alexitímia Skála (TAS-20) magyar változata: Megbízhatósága és faktorvaliditása egyetemista mintán [Hungarian version of the Toronto Alexithymia Scale (TAS-20): Reliability and factor validity in a student sample]. Magyar Pszichológiai Szemle, 62. https://doi.org/10.1556/mpszle.62.2007.3.4
TAS-20 - Indonesian
TAS-20 - IndonesianGeni, P. (2020). Struktur Internal dan Validitas Konstruk dari Toronto Alexithymia Scale (TAS-20) dengan Sampel Mahasiswa pada Universitas di Jakarta. JP3I (Jurnal Pengukuran Psikologi dan Pendidikan Indonesia), 9(1), 30-40. https://doi.org/10.15408/jp3i.v9i1.15450
TAS-20 - Italian
TAS-20 - ItalianBressi, C. et al. (1996) Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: An Italian multicenter study. Journal of Psychosomatic Research, 41(6), 551-559. https://doi.org/10.1016/S0022-3999(96)00228-0
TAS-20 - Japanese
TAS-20 - JapaneseKomaki, G., Maeda, M., Arimura, T., Nakata, A., Shinoda, H., OgataI Shimura, M., Kawamura, N., & Kubo, C. (2003) The reliability and factorial validity of the Japanese version of the 20-item Toronto Alexithymia Scale. Journal of Psychosomatic Research, 55(2), 143. https://doi.org/10.1016/S0022-3999(03)00360-X
Moriguchi, Y., Maeda, M., Igarashi, T. et al. (2007) Age and gender effect on alexithymia in large, Japanese community and clinical samples: a cross-validation study of the Toronto Alexithymia Scale (TAS-20). BioPsychoSocial Med 1, 7. https://doi.org/10.1186/1751-0759-1-7
TAS-20 - Korean
TAS-20 - KoreanWoon-Sun Jeong, et al. (2003). Comparison of Reliability and Validity of Three Korean Versions of the 20-Item Toronto Alexithymia Scale. Psycho-Physical Medicine, 11(1), 77 - 88.
TAS-20 - Latvian
TAS-20 - LatvianLaura Bubko, Annija Mežmača, Inese Jurķāne, Zane Lucāne, Artūrs Ancāns “TORONTO – ALEXITHYMIA SCALE 20” SCORES AMONG PSYCHIATRIC PATIENTS COMPARED TO OTHER INPATIENTS. PROCEEDINGS OF THE 58th INTERNATIONAL SCIENTIFIC CONFERENCE OF DAUGAVPILS UNIVERSITY.
TAS-20 - Lithuanian
TAS-20 - LithuanianBeresnevaitė, M., Taylor, G.J., Parker, J.D.A., & Andziulis, A. (1998). Cross validation of the factor structure of a Lithuanian translation of the 20-item Toronto Alexithymia Scale. Acta Medica Lituanica, 5(2): 146-149.
TAS-20 - Macedonian
TAS-20 - MacedonianPop-Jordanova, N., Polenakovic, M., Pop-Jordanov, J., Shaltanovska, H., & Trajceska, L. (2013). Are Macedonian chronic patients alexithymic? Prilozi (Makedonska Akademija na Naukite i umetnostite. Oddelenie za Medicinski Nauki), 34(3), 31-38.
Pop-Jordanova N, Boskovska V. (1995). TAS-20 as a measure of alexithymia in Macedonian population. Neurologia Croatica, 44(1), 60.
TAS-20 - Norwegian
TAS-20 - NorwegianPedersen, G., Normann-Eide, E., Eikenaes, I. U., Kvarstein, E. H., & Wilberg, T. (2021 in press). Psychometric evaluation of the Norwegian Toronto Alexithymia Scale (TAS-20) in a multisite clinical sample of patients with personality disorders and personality problems. Journal of clinical psychology. https://doi.org/10.1002/jclp.23270
TAS-20 - Persian/Farsi
TAS-20 - Persian/FarsiBesharat, M. A. (2007). Reliability and Factorial Validity of a Farsi Version of the 20-Item Toronto Alexithymia Scale with a Sample of Iranian Students. Psychological Reports, 101(1), 209–220. https://doi.org/10.2466/pr0.101.1.209-220
Besharat, M. (2008). Psychometric Characteristics of Persian Version of the Toronto Alexithymia Scale-20 in Clinical and Non-Clinical Samples. Iranian Journal of Medical Sciences, 33(1), 1-6.
TAS-20 - Polish
TAS-20 - PolishŚcigała, D.K., Zdankiewicz-Ścigała, E., Bedyńska, S. & Kokoszka, A. (2020) Psychometric Properties and Configural Invariance of the Polish – Language Version of the 20-Item Toronto Alexithymia Scale in Non-clinical and Alcohol Addict Persons. Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2020.01241
Ścigała, Dawid & Zdankiewicz-Ścigała, Elżbieta & Bedyńska, Sylwia & Kokoszka, Andrzej. (2020). Toronto Alexithymia Scale TAS -20 PL. The Polish TAS-20 is available on researchgate.
TAS-20 - Portuguese
TAS-20 - PortugueseVerissimo R. (2001). Versão Portuguesa da Escala de Alexitimia de Toronto de 20-itens--I. Adaptação linguística, validação semântica, e estudo de fiabilidade [The Portuguese version of the 20-item Toronto Alexithymia Scale -- I. Linguistic adaptation, semantic validation, and reliability study]. Acta medica portuguesa, 14(5-6), 529–536.
Stivaleti Colombarolli, M., Carolina Zuanazzi, A., Koich Miguel, F., & Giromini, L. (2019). Psychometric properties of the Toronto Alexithymia Scale (TAS-20) in Brazil. Transcultural Psychiatry, 56(5), 992–1010. https://doi.org/10.1177/1363461519847312
TAS-20 - Romanian
TAS-20 - RomanianRaluca A. Morariu, Lindsay E. Ayearst, Graeme J. Taylor, R. Michael Bagby (2013). DEVELOPMENT AND VALIDATION OF A ROMANIAN ADAPTATION OF THE 20-ITEM TORONTO ALEXITHYMIA SCALE (TAS-20-RO). Revista Romana de Psihiatrie, 4. Full text of the article is available on www.romjpsychiat.ro
TAS-20 - Russian
TAS-20 - RussianStarostina, E. G., Taylor, G. D., Quilty, L. K., Bobrov, A. E., Moshnyaga, E. N., Puzyreva, N. V., Bobrova, M. A., Ivashkina, M. G., Krivchikova, M. N., Shavrikova, E. P., & Bagby, M. (2010). Торонтская шкала алекситимии (20 пунктов): валидизация русскоязычной версии на выборке терапевтических больных [Toronto Alexithymia Scale (20 points): validation of the Russian-language version on a sample of therapeutic patients]. Social and Clinical Psychiatry, 20(4), 31–38.
TAS-20 - Serbian
TAS-20 - SerbianTrajanovic, N., Djurić, V., Latas, M., Milovanović, S., Jovanović, A., & Djurić, D. (2013). Serbian translation of the 20-item Toronto Alexithymia Scale: psychometric properties and the new methodological approach in translating scales. Srpski arhiv za celokupno lekarstvo, 141 5-6, 366-70. http://doi.org/10.2298/SARH1306366T
The Serbian translation of the 20-item Toronto Alexithymia Scale is in Appendix I. The full text of the article is available on www.semanticscholar.org
TAS-20 - Slovak
TAS-20 - SlovakLÁTALOVÁ, V. & PILÁRIK, Ľ. (2015) OVERENIE RELIABILITY A FAKTOROVEJ VALIDITY SLOVENSKEJ VERZIE DOTAZNÍKA TORONTO ALEXITHYMIA SCALE-20 NA SÚBORE SLOVENSKÝCH ŠTUDENTIEK. Ceskoslovenska Psychologie, 59, 4,369-379.
TAS-20 - Somali
TAS-20 - SomaliReferences:
Kankaanpää, S. (2017). Mental Health Among Somali Origin Migrants in Finland. Dissertation: University of Tampere.
TAS-20 - Spanish
TAS-20 - SpanishGonzález-Arias, M., Martínez-Molina, A., Galdames , S., Urzúa, A. (2018) Psychometric Properties of the 20-Item Toronto Alexithymia Scale in the Chilean Population. Frontiers in Psychology, 9, 963. https://doi.org/10.3389/fpsyg.2018.00963 The TAS-20 Spanish version is in Table 1.
Fernández-Jiménez, E., Pérez-San-Gregoria, A., Taylor, G.J., Bagby, R.M., Ayearst, L.E., Izquierdo, G. (2013). Psychometric properties of a revised Spanish 20-Item Toronto Alexithymia Scale adaptation in multiple sclerosis patients. International Journal of Clinical and Health Psychology, 13, 226-234.
TAS-20 - Swedish
TAS-20 - SwedishSimonsson-Sarnecki, M., Lundh, L. G., Törestad, B., Bagby, R. M., Taylor, G. J., & Parker, J. D. (2000). A Swedish translation of the 20-item Toronto Alexithymia Scale: cross-validation of the factor structure. Scandinavian journal of psychology, 41(1), 25–30. https://doi.org/10.1111/1467-9450.00167
TAS-20 - Turkish
TAS-20 - TurkishGüleç, Hüseyin & Kose, Samet & Yazici, Medine & Çıtak, Serhat & Evren, Cuneyt & Borckardt, Jeffrey & Sayar, Kemal. (2009). The Turkish Version of the 20-Item Toronto Alexithymia Scale (TAS-20): Reliability, Validity, and Factorial Structure. Bulletin of Clinical Psychopharmacology, 19, 214-220.
The Turkish Translation of the TAS-20 is in the Appendix. The full text of the article is available on halileksi.net
TAS-20 - Urdu
TAS-20 - UrduSaba Ghayas, Sadia Niazi, Maria Ghazal and Wajeeha Tahir (2017) Urdu Translation and Validation of Toronto Alexithymia Scale. Journal of the Indian Academy of Applied Psychology, 43(1), 114-12
Computerized measures
Computerized measuresIn this page I have uploaded a series of computerized measures that I have written in Visual Basic for Applications and used in a few studies. One of these measures, the Deictic Relational Task is a deictic framing measure that captures both deictic accuracy and fluency. We have been developing this measure over the last years with Michael Levin, Steven C. Hayes, Colin Stromberg and others.
There are many advantages to use Microsoft PowerPoint to write your computerized questionnaires and tasks. First of all, it is a highly disseminated software that I think most of you have. Secondly, it can potentially reduce acquiescence bias since you can change the background and format of each measure and you will be more likely to keep the participant's attention throughout.
The code of these slides (which you can find if you add the developer tab under options and click "visual basic") is freely available for modification and improvement as long as your intent is to benefit your clients, research and/or for enhancing the work of other scientist practitioners and researchers. Please, feel free to contact me if you find ways to improve the visual basic code or for questions about it. If you have questions about how to score the Deictic Relational Task or about how to compile all the measures together in a single PowerPoint document, let me know as well.
Note: make sure you enable macro before you try the measure (ex: Powerpoint Options/Trust Center/Trust Center Settings/Macro Settings/Enable all macros).